Authored by Dr. Angie RombolaBackground:
Clinical Features:
0 Comments
By: DR. AUSTIN COSTA
Management:
References
Authored by: Blake Bauer, MD
The Foot
The Ankle and Lower Leg
The Knee
The Hip
Authored by Dr. Javier Andrade
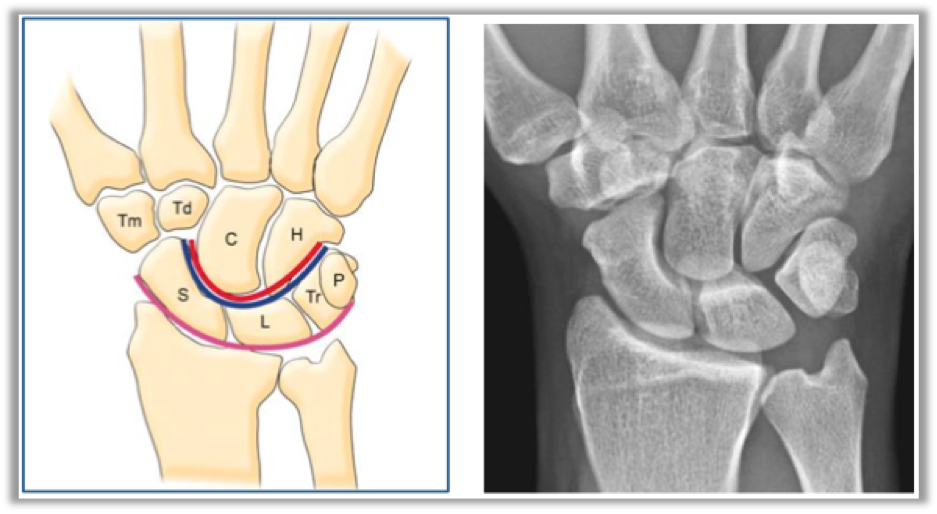
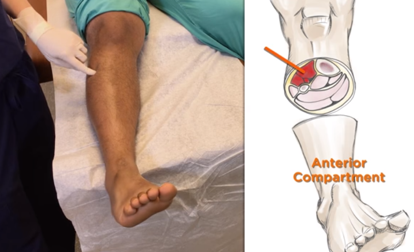
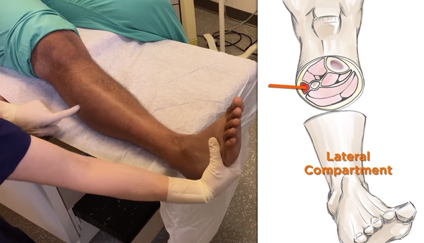
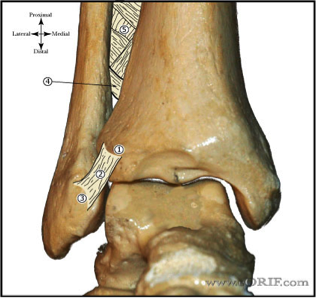
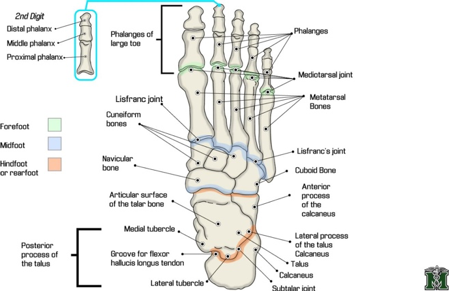
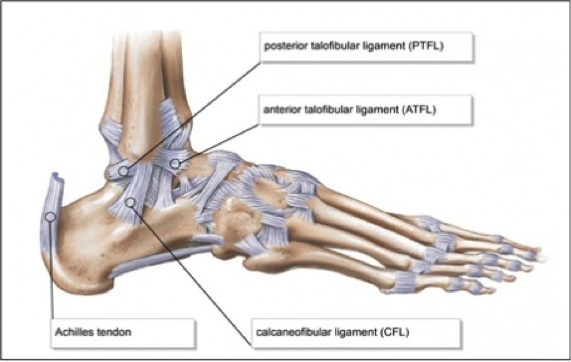
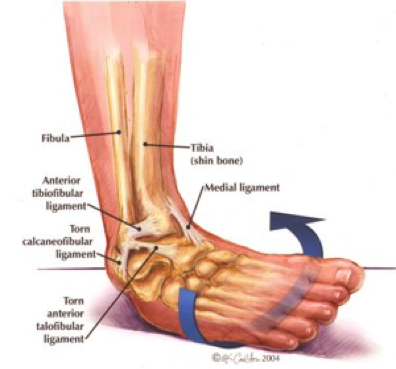
Authored by Dr. Jessica Hoglund 1. Differential (categorized based on gait pattern) A. Antalgic gait 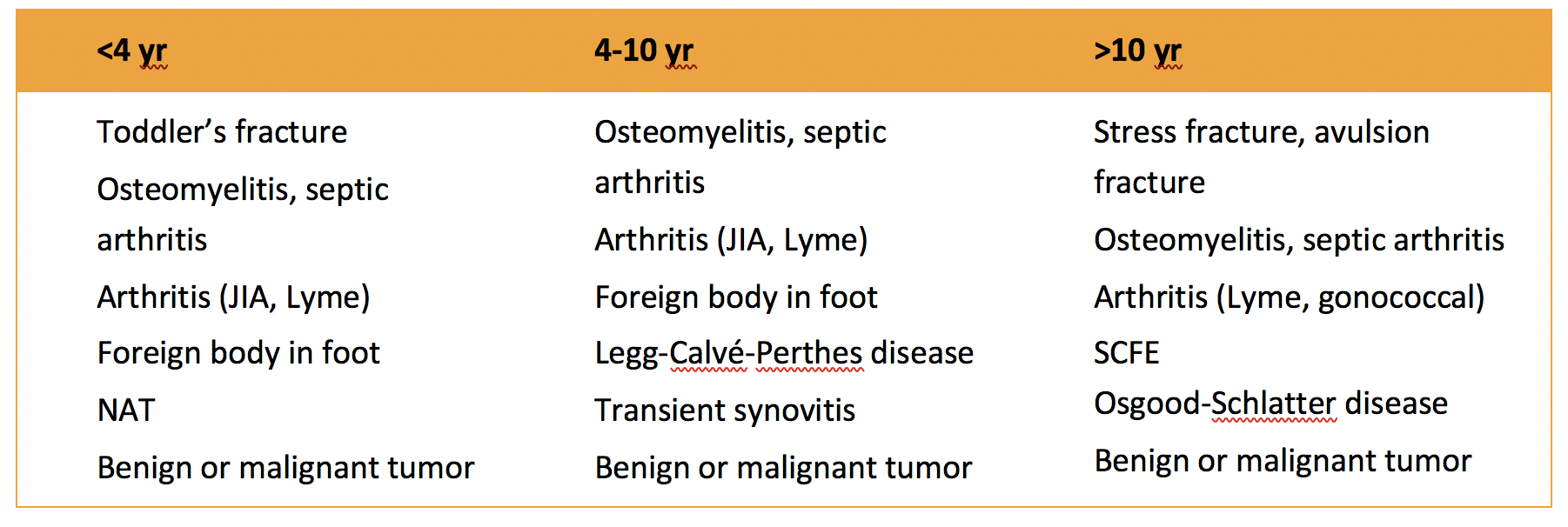 B. Non-antalgic gait 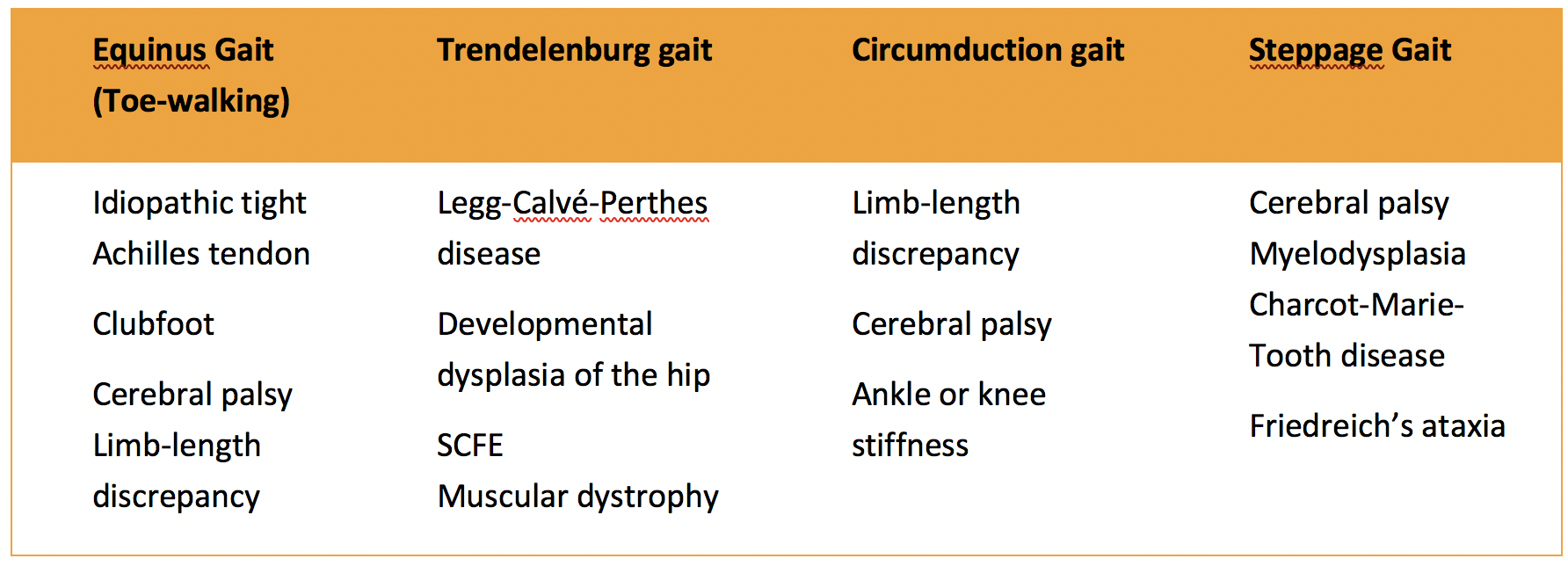 1. Transient synovitis A. Most common cause of hip pain/limp in children <10 yrs B. Aseptic inflammation of the hip (postviral etiology) C. Diagnosis i. Physical exam: 1. Non-toxic 2. Antalgic gait i. Imaging performed when considering other differentials ii. Ultrasound may be performed to confirm the presence of a joint effusion D. Management i. Rest ii. Analgesics 2. Septic arthritis A. Causes i. Bacterial infection of joint ii. Most commonly s. aureus iii. Consider E. coli or GBS in children < 2 months iv. Consider gonococcal arthritis in adolescents, sexually active patients, and in polyarticular arthritis v. Consider salmonella in sickle cell disease B. Clinical features i. Neonates often do not appear ill and may not have fever in 50% of cases ii. Older infants, toddlers, children may localize, limp, or refuse to walk C. Diagnosis i. Physical exam1. Limb externally rotated, flexed, and abducted ii. Labs1. CBC, ESR, possibly blood cultures iii. Kocher criteria (septic arthritis vs transient synovitis, >3 predictors high risk for septic arthritis) 1. Non weight-bearing 2. Temp > 101.3oF (38.5oC) 3. ESR > 40 mm/hr 4. WBC > 12,000 cells/mm3 iv. Imaging  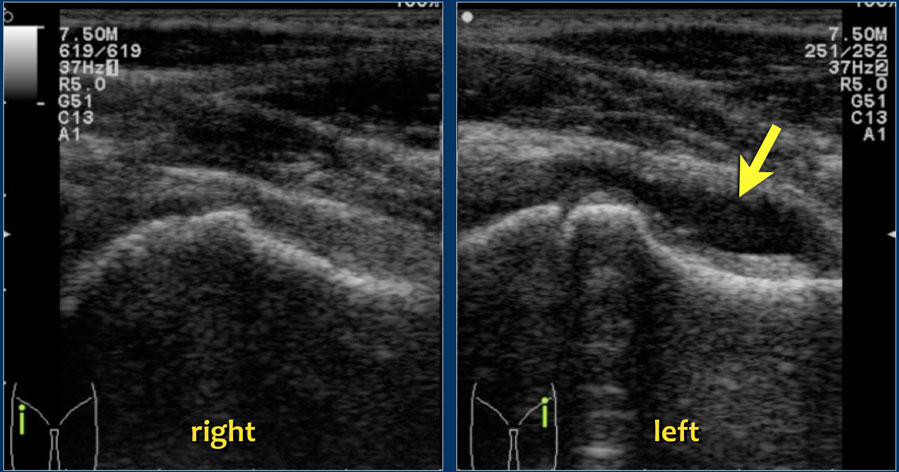 v. Arthrocentesis 1. Ultrasound guided or fluoro guided for hip 2. Synovial fluid with >50,000 WBC’s, >75% PMN’s, positive gram stain and culture D. Management i. IV antibiotics (vanc, rocephin or cefoxatime if < 2 months) ii. Surgical drainage E. Complications i. Avascular necrosis ii. Capsule damage iii. Chronic arthritis iv. Osteomyelitis v. Sepsis 4. SCFE A. MCC of hip disability in adolescents B. Obese adolescents whose hips are exposed to repetitive minimal trauma C. Diagnosis i. Physical exam 1. Decreased internal rotation 2. Antalgic or Trendelenburg gait 3. Determine if pt is able to ambulate with or without crutches (determines prognosis) ii. Imaging 1. Any adolescent with chronic groin, hip, thigh, or knee pain deserves bilateral hip XR (AP and lateral) 2. High incidence of bilateral disease 3. Use Klein’s lines to aid in diagnosis. A and C below are abnormal. B and D are normal (line drawn from superior aspect of femoral neck transects lateral aspect of femoral head). 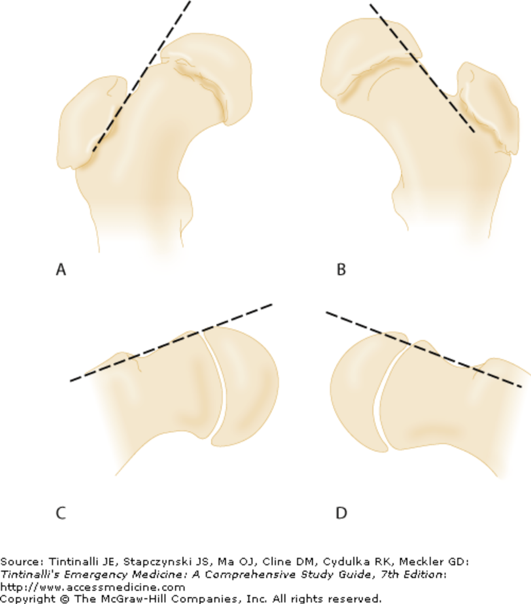  D. Management i. Non weight bearing (important to prevent further slippage) ii. Operative management with possible prophylactic pinning of contralateral hip E. Complications i. Avascular necrosis ii. Premature closure of physis iii. Limited ROM iv. Osteoarthritis 5. Legg-calve-perthes disease A. Idiopathic avascular necrosis of proximal femoral epiphysis B. Usually unilateral (10-15% bilateral) C. Clinical features i. Insidious onset of mild hip or knee pain, possible limp ii. Repeated episodes of ischemia of femoral head à infarction and necrosis à subchondral stress fracture D. Diagnosis i. Physical exam 1. Decreased abduction and internal rotation 2. Possible thigh atrophy on affected side 3. Limb shortening (advanced cases) ii. Imaging 1. Early radiographs may be normal, but MRI will show edema in femoral epiphysis with T1 weighted 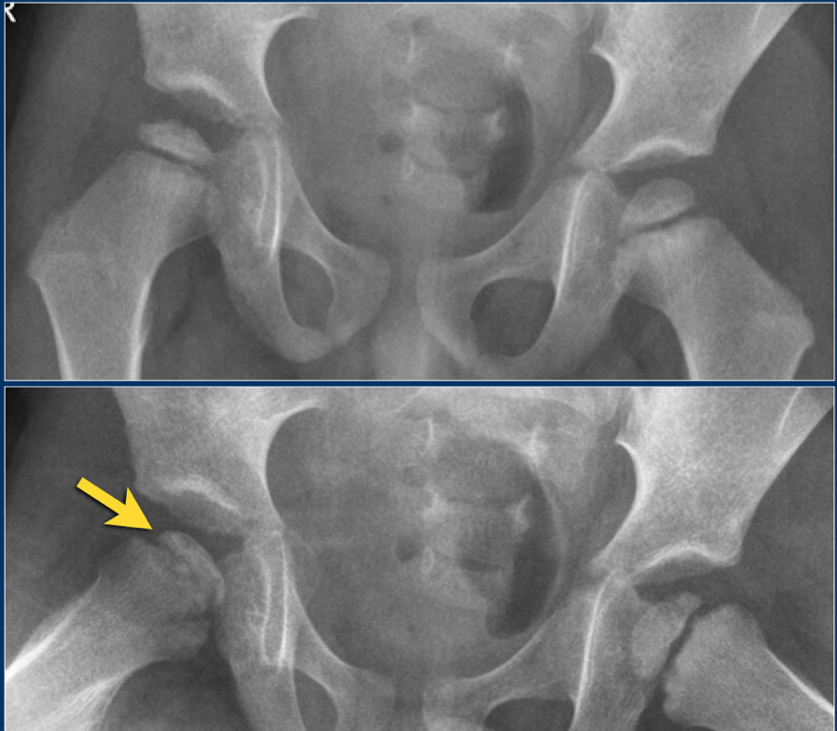 2. Radiographic progression of disease 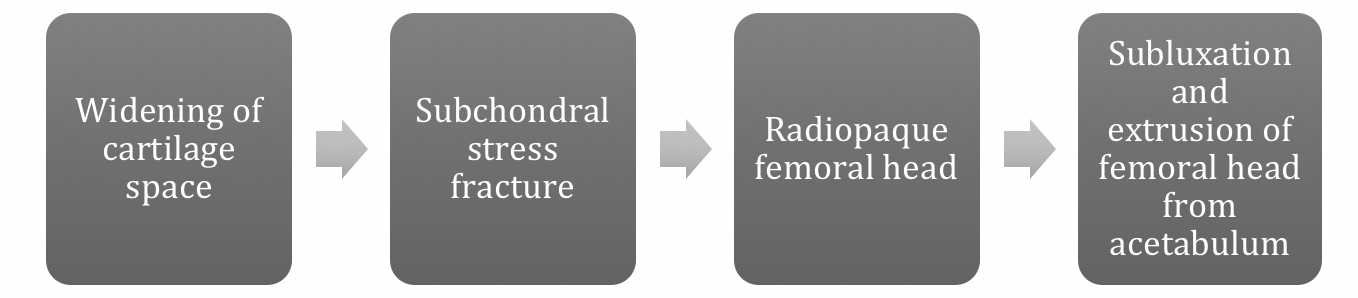 E. Management i. Symptomatic tx ii. Non weight bearing iii. Operative management may prevent early osteoarthritis can be managed non-operatively with spontaneous revascularization of femoral head F. Complications i. Osteoarthritis ii. Coxa magna deformity (short, broad femoral head and column)  Flynn, John M, and Roger F Widmann. “The Limping Child: Evaluation and Diagnosis.” Journal of the American Academy of Orthopaedic Surgeons, vol. 9, no. 2, Apr. 2001.Horowitz, Diane Lewis, et al. “Approach to Septic Arthritis.” American Family Physician, 15 Sept. 2011, www.aafp.org/afp/2011/0915/p653.html.“Imaging in Slipped Capital Femoral Epiphysis .” Imaging in Slipped Capital Femoral Epiphysis: Practice Essentials, Radiography, Computed Tomography, 6 May 2017, emedicine.medscape.com/article/413810-overview.“Legg-Calve-Perthes.” Legg-Calve-Perthes - Orthopedics - Medbullets Step 2/3, step2.medbullets.com/orthopedics/120519/legg-calve-perthes.Radiology In Ped Emerg Med, Vol 4, Case 17, www.hawaii.edu/medicine/pediatrics/pemxray/v4c17.htmlSwaminathan, Anand. “Pediatric Septic Hip.” Core EM, coreem.net/core/pediatric-septic-hip/.Tintinalli JE, Stapczynski J, Ma O, Cline DM, Cydulka RK, Meckler GD, T. Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 7e; 2011 Available at:http://accessmedicine.mhmedical.com/content.aspx?bookid=348§ionid=40381606 Accessed: February 12, 2018 In order to begin an appropriate assessment of the ankle, it is necessary to review the significant anatomical structures. Bony Anatomy First, we have the two long bones that form the proximal portion of the joint – the tibia and the fibula. At the ankle joint, the tibia extends as the lateral malleolus and posterior malleolus while the fibula forms the medial malleolus. The distal boney structure of the joint is formed by the talus. 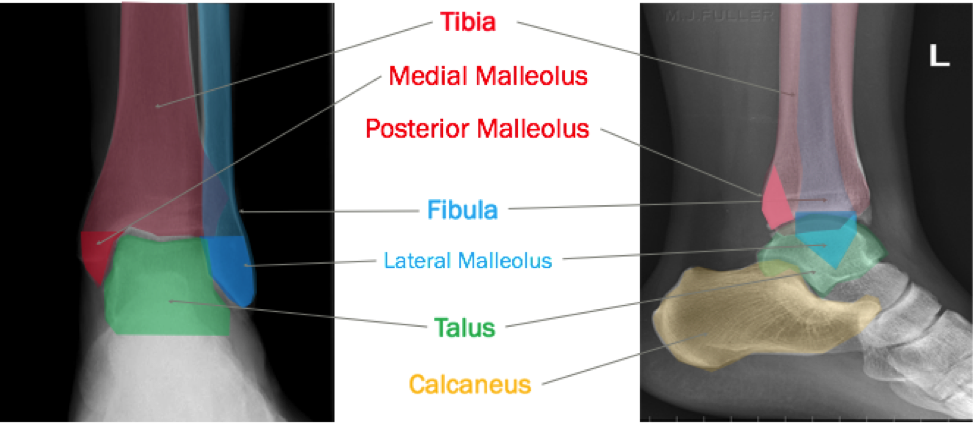 Joint Anatomy A majority of the articular surface is formed by the horizontal portion of the distal tibia (the tibial plafond) which extends parallel to the dome of the talus; taken with the medial and lateral malleoli, it forms a rectangular socket known as the ankle mortise. Being a synovial joint, the ankle joint (between the ankle mortise and talar dome) is surrounded by a joint capsule. Like the knee joint capsule, the ankle capsule has an additional cranial extension at the syndesmosis. 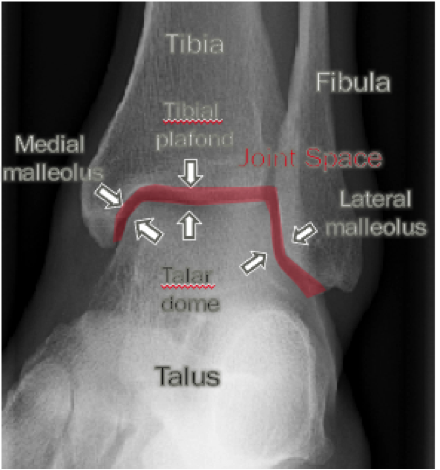 Ligament Anatomy The lateral and medial malleoli have ligamentous attachments to the talus and calcaneus that contribute to stability of the joint.

 Initial Evaluation A patient presenting with a suspected ankle injury should undergo the following assessment:
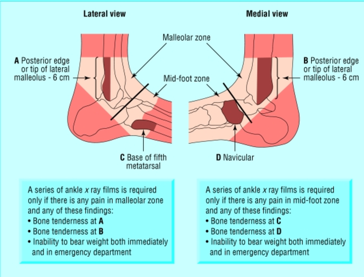
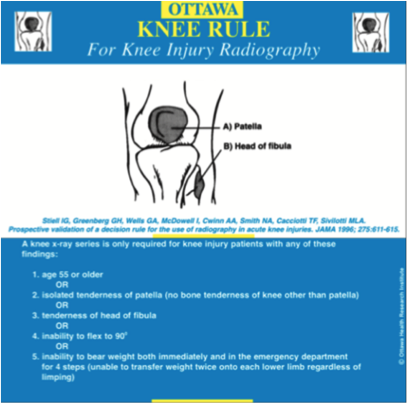
Our initial evaluation is important because it helps utilize the following decision tool: Ottawa Ankle Rule The Ottawa Ankle Rule helps us screen for patients that will benefit from ankle imaging. Ankle Imaging is warranted in those who have ankle pain and:
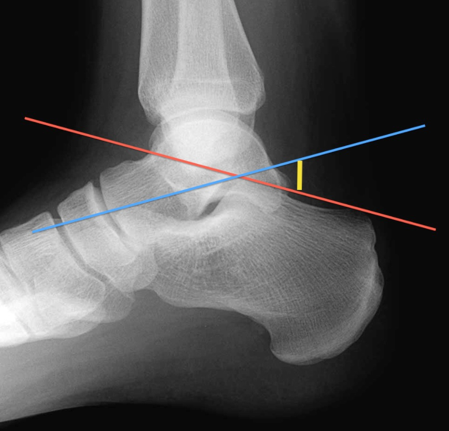
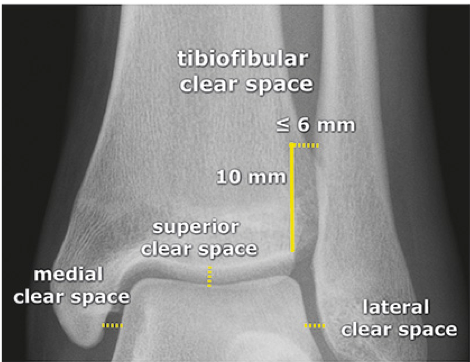
Tips from the creators at University of Ottawa: Palpate the entire distal 6cm of the fibula and tibia; Do not neglect the importance of medial malleolar tenderness; “Bearing weight” counts even if the patient limps; Be caution in patients under age 18. Imaging Studies When imaging the ankle obtain 3 views to appropriately evaluate the joint: AP, Lateral and the Mortise study.  Radiographic Evaluation Begin with the AP and Lateral views. Trace the entire length of the tibia and fibula paying special attention to the fibula on the lateral view, for oblique fractures may be difficult to see. Next, proceed to the mortise view. Trace around the mortise and Talar dome, evaluate for joint space uniformity. The ring structure of the ankle is made up of three bones (tibia, fibula and talus) and three ligaments (medial and lateral collateral ligaments and interosseous ligament) if there is one break in the ring, look for a second. To evaluate the integrity of the syndesmosis use the following measurements: •Tibiofibular overlap < 1mm •Increased medial clear space: less than or equal to 4 mm •Increased Tibiofibular clear space: < 6 mm  Additional radiographic measurements Talo-crural angle : The angle is formed by drawing a line parallel to the tibial plafond, a line perpendicular to the tibail plafond, and a line connecting the lateral and medial malleoli. This angle should be between 75 – 87 degrees and should be within 2-5 degrees of contralateral side. Deviation from these measurements is indicative of fibula shortening.  Typical Fracture Patterns Isolated Medial Malleolus Fracture 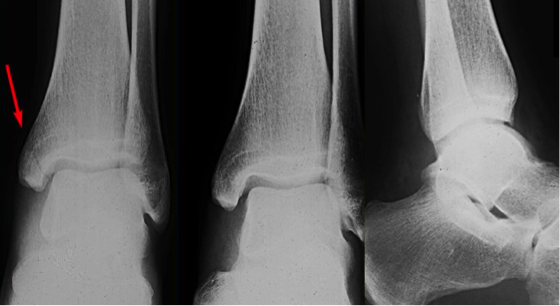 Isolated Lateral Malleolus Fracture  Isolated Posterior Malleolus Fracture  Bimalleolar fracture / equivalent  *Notice how there are two breaks to the ring structure, therefore this injury pattern is consistent with an unstable joint (increased medial clear space, distal fibula fracture). These unstable injuries convey a higher need for orthopedic intervention. Associated syndesmotic injuries
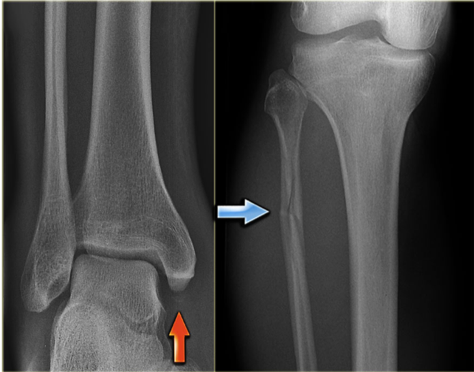
Pilon Fracture This following fracture pattern is often confused for an ankle fracture, however the presence of a pilon fracture conveys a different mechanism and prognosis. A Pilon fracture, French for mortar and pestle, occurs due to an axial loading mechanism and is defined by articular impaction and comminution of the distal tibia. When you see a pilon fracture it is important to evaluate for other injuries typical of axial loading (i.e. lumbar spine, calcaneus, ect.) 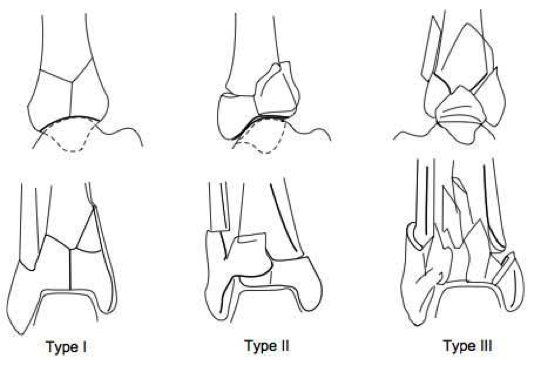
Sources https://radiopaedia.org/articles/ankle-radiograph-an-approach http://www.orthobullets.com/trauma/1047/ankle-fractures http://www.orthobullets.com/trauma/1046/tibial-plafond-fractures?expandLeftMenu=true https://radiopaedia.org/search?utf8=✓&q=pilon+fracture&scope=all https://meds.queensu.ca/central/assets/modules/ts-ankle-radiograph/isolated_medial_malleolus_fracture.html BY: DR. ETHEN ELLINGTON M.D.
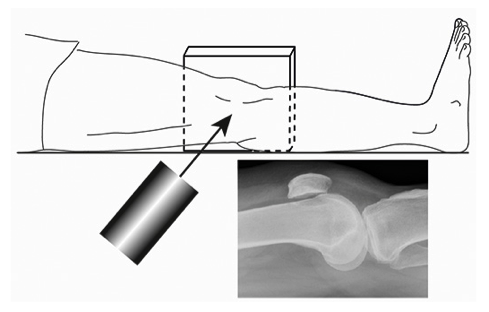
Standard Views:
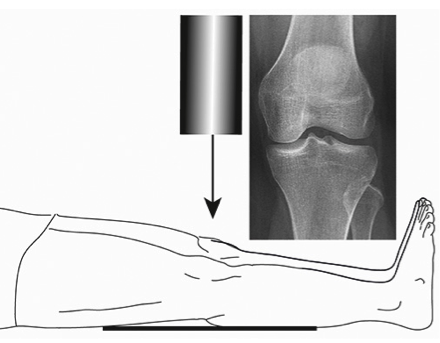
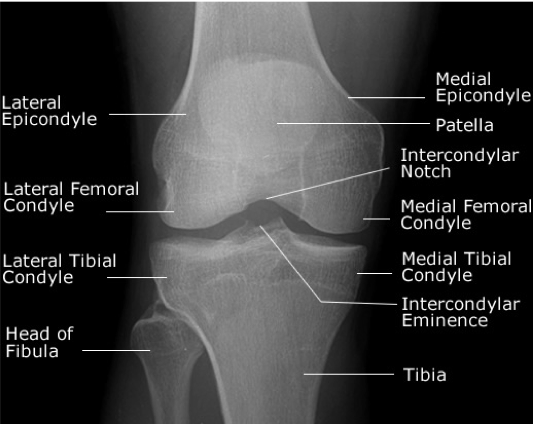
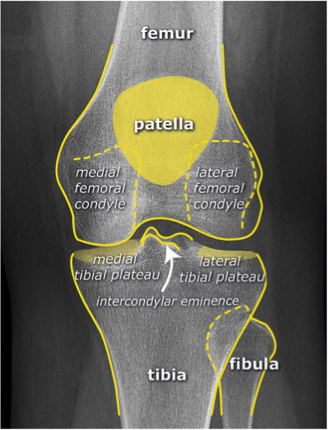
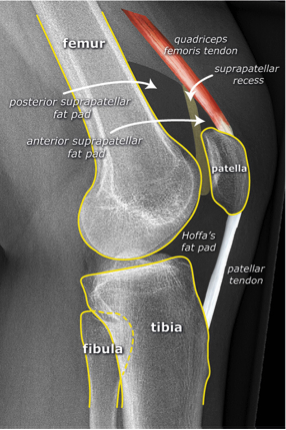
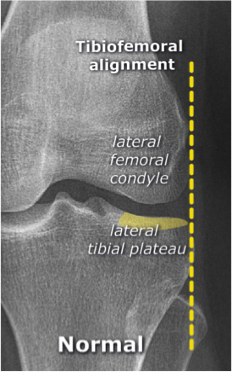
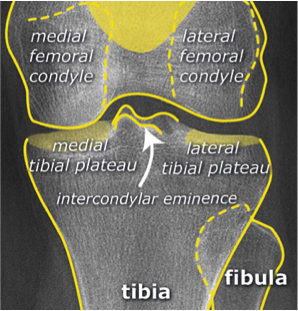
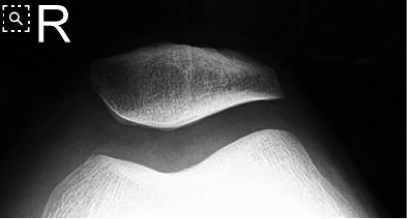 Systematic Approach to Adult Knee Films: 1) Know your anatomy!
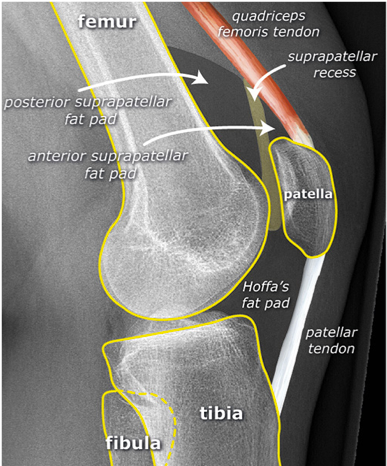
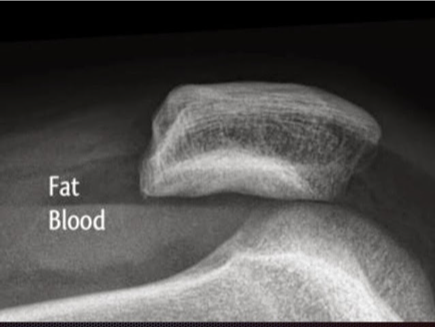
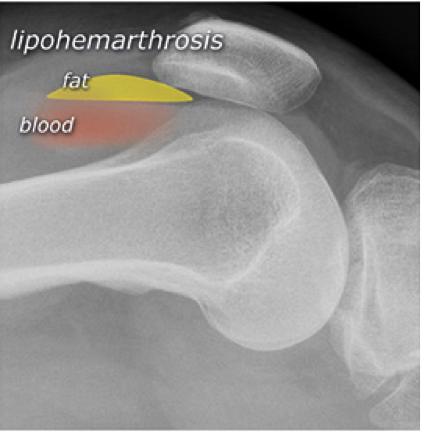
2) Check for an effusion
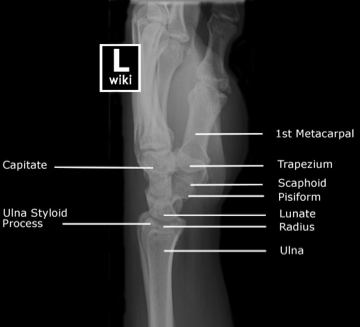
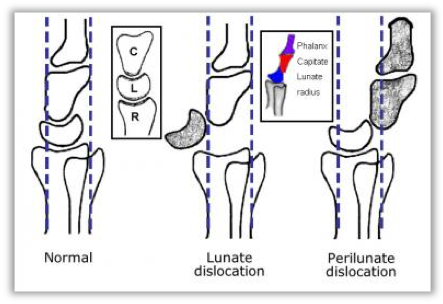
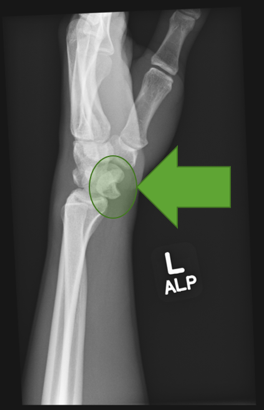
7) Don’t forget the fabella! It’s a normal sesamoid bone of the lateral head of gastrocnemius tendon - NOT to be mistaken for a fracture or loose body 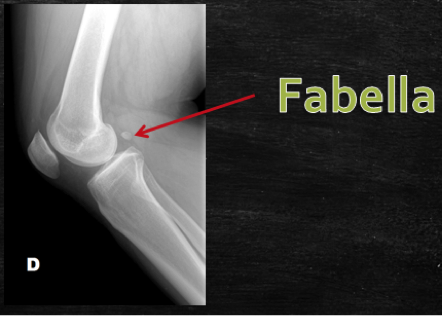 Resources and Images: https://radiopaedia.org/articles/knee-series https://radiopaedia.org/articles/knee-radiograph-an-approach http://dontforgetthebubbles.com/knee-x-ray-interpretation/ http://www.radiologymasterclass.co.uk/tutorials/musculoskeletal/x-ray_trauma_lower_limb/knee_x-ray http://www.imageinterpretation.co.uk/knee.php By: Dr. jeremy driscoll M.D. Volar Splint Indications: -Hand and Wrist injures (NOT distal radius or ulna fractures, can still supinate and pronate) -Carpal fractures -Lunate dislocation -2nd-5th metacarpal head fracture Application: -Extends along volar forearm from metacarpal heads to just proximal to radial head -Allow flexion of elbow -Wrist at 20 degrees of extension -Can add dorsal "sandwich" for stability Ulnar Gutter Splint Indications: -4th and 5th phalanges and metacarpals Application: -Extends from 5th DIP to proximal forearm -Wrist at 20 degrees of extension -Flex MCPs at 50-70 degrees, PIP and DIPs in slight flexion Thumb Spica Splint Indications: -Scaphoid and lunate fractures -1st metacarpal fracture -Thumb fractures -De Quervain tenosynovitis Application: -Extends from tip of thumb to proximal forearm -Wrist at 20 degrees of extension -Thumb slightly flexed Long Arm Splint Indications: -Proximal forearm and elbow fractures -Intraarticular fractures of distal humerus and olecranon Application: -Elbow at 90 degrees of flexion -Neutral forearm and wrist 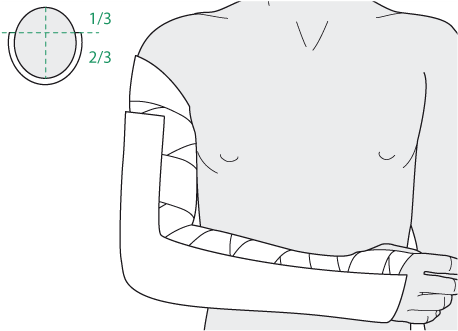 Sugar Tong Splint Indications: -Wrist and distal forearm fractures Application: -Extends from MCPs on dorsum, around elbow, to volar midpalmar crease -Elbow at 90 degrees of flexion -Neutral forearm and wrist -Double sugar tong for complex or unstable forearm and elbow fractures Resources:
Michael T Fitch, MD. Basic Splinting Techniques. New England Journal of Medicine. 2008; 359:e32. Wikiem.com Ortho-teaching.feinberg.northwestern.edu/docs/Splinting.pptx HPI: 23 yo male s/p MCC. Patient reports that he swerved to avoid hitting a vehicle in front of him that stopped abruptly and layed down his bike, landing on his right shoulder. He was helmeted and did not lose consciousness. Ambulatory after the event, hemodynamically stable, and complaining of right shoulder pain. Exam:  Radiology: 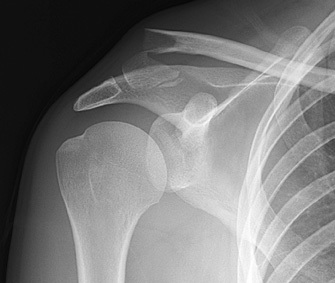 Management: Middle Third (80-85%) 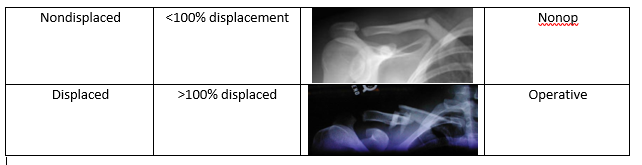 Lateral Third (10-15%) 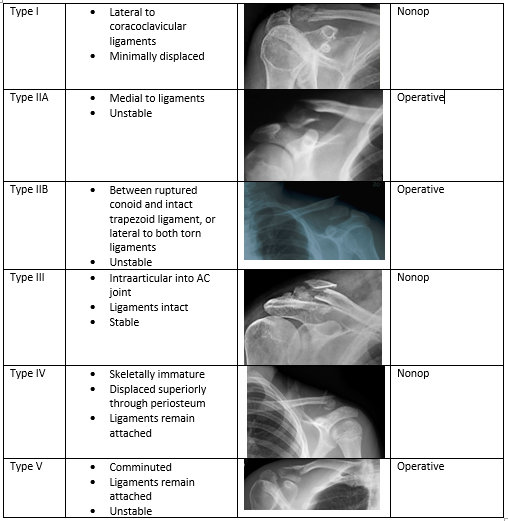 Medial Third (5-8%)  Treatment:
Nonop
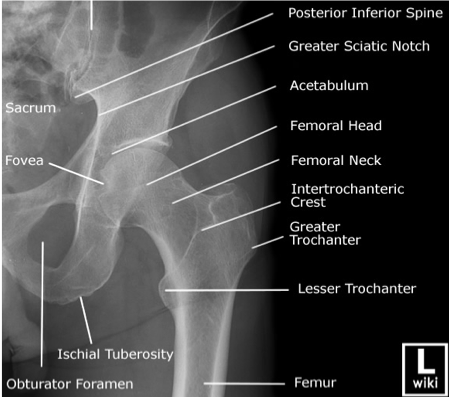
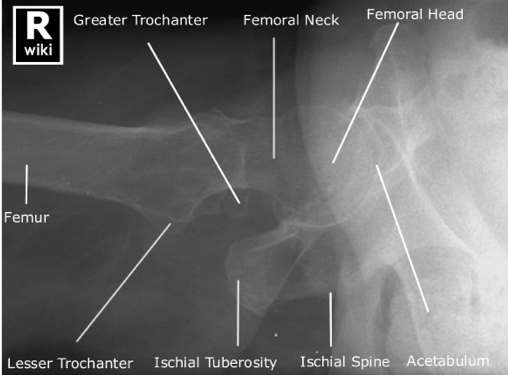
Resources: Orthobullets.com HPI: 22 yo otherwise healthy male presents s/p head on MVC vs tree. Patient is awake and alert, hemodynamically stable, complaining of right hip pain. Physical Exam: No external signs of trauma. Right lower extremity is shortened compared to the left and internal rotated. No numbness, 2+ DP pulse.   Classification: - Simple: pure dislocation - Complex: with associated fracture of acetabulum or proximal femur Mechanism: - Axial load on femur while hip flexed and adducted or through flexed knee (dashboard injury such as this patient) Requires emergent reduction (within 6 hours!) due to risk of vascular compromise to hip and osteonecrosis However... Examine femoral neck closely on XR to rule out fracture prior to attempting closed reduction. With ipsilateral femoral neck fracture, closed reduction is contraindicated! 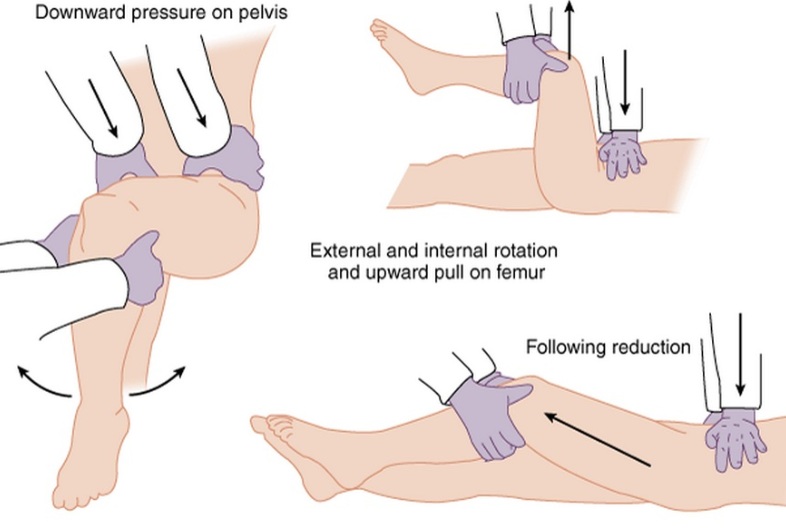 Patient must be adequately sedated for procedure. Propofol helps with tissue relaxation! Post reduction CT must be performed to evaluate for: - femoral head fractures - loose bodies - acetabular fractures Commonly associated with ipsilateral knee injuries (up to 25%) Dispo: For simple dislocation, protected weight bearing for 4-6 weeks Resources: 1. Serna, Fernando MD, Corczyca, John MD. Hip Dislocations and Femoral Head Fractures. University of Rochester Medical Center. March 2004. 2. Orthobullets.com |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|

























 RSS Feed
RSS Feed
