|
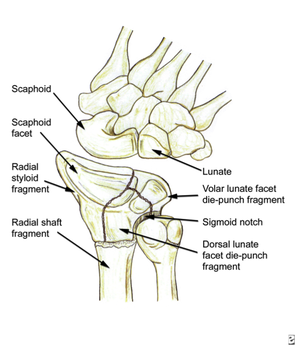
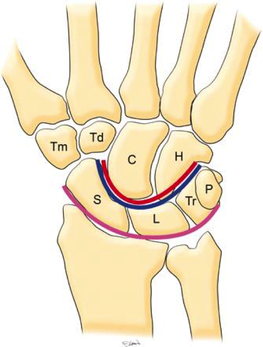
HPI: Young male presents after a fall while skiing with right shoulder and wrist pain. PE: Obvious deformity of the right wrist. No abrasions or ecchymosis. Full thumb abduction, able to flex at DIP and PIP joint of all 5 fingers, full abduction of all 4 palmar fingers, 5/5 strength to finger grip. Unable to range wrist, elbow or glenohumeral joint secondary to pain. Normal sensation to pinprick and two point discrimination of all five fingers. 2+ radial pulse with normal cap refill. Imaging:  Anatomy: - Normal wrist anatomy consists of two rows of bones: o Proximal row: Scaphoid, lunate, triquetrum, pisiform o Distal row: trapezium, trapezoid, capitate, hamate - Ligaments of the wrist: o Interosseous ligaments run between the carpal bones and stabilizes proximal carpal bones. o Intrinsic ligaments insert and originate among the carpal bones to internally stabilize them. o Extrinsic ligaments connect radius and ulna to the carpus.
How to make diagnosis:
Treatment: o Require emergent closed reduction and splinting into sugar tong splint.
Pearls:
0 Comments
HPI: Adult male presents after being involved in a motor vehicle collision with right wrist pain and obvious distal deformity. PE: Obvious deformity of the right wrist. No abrasions or ecchymosis. Full thumb abduction, able to flex at DIP and PIP joint of all 5 fingers, full abduction of all 4 palmar fingers, 5/5 strength to finger grip. Slightly limited range of motion to flexion or extension wrist secondary to pain. Significant pain with pronation and supination. Normal sensation to pinprick and two point discrimination of all five fingers. 2+ radial pulse with normal cap refill. Imaging: 
How to Diagnosis: Radial shaft fracture and concurrent distal radioulnar joint. Most commonly seen in fractures of the distal 1/3 of the radius. Termed a Galeazzi fracture. Typically occurs secondary to direct wrist trauma (most classically dorsolateral) or with fall onto outstretched hand with forearm in pronation. Anatomy:
Treatment:
Pearls:
HPI: Middle age male who presents after falling at work. His medial forearm stroke a metal bucket just distal to his elbow and resulted in a large laceration. PE: Patient is unable to flex at the DIP of digit 4 and 5. He is unable to cross the second and third fingers or adduct his fingers. He has decreased sensation over the medial aspect of the 4th and 5th digit. Suspected ulnar nerve laceration.  Anatomy: Derives from the medial portion of the brachial plexus (C8-T1). It lies posteromedial to the brachial artery in the upper arm and traverses behind the medial epicondyle. The ulnar nerve runs along on the ulnar aspect of the wrist along with the ulnar artery. It passes through Guyon’s canal where it bifurcates into sensory and deep motor branches. 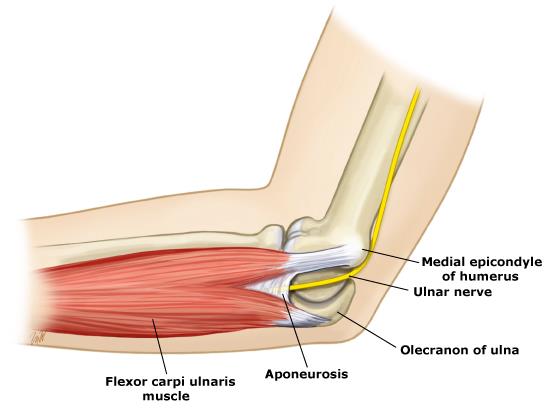 Innervation:
- Motor:
- Sensory:
Clinical conditions:
Treatment: Forearm exploration with transected nerve repair. Pearls:
|
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|

 RSS Feed
RSS Feed
