hpiA 15 yr old female right hand dominant with no significant past medical history presents with left shoulder pain after sustaining injury while playing basketball. States she can not clearly recall the events but remembers extending her arm for the ball and having sudden onset of pain. Describes generalized constant aching pain to the left shoulder only. She has been unable to range her left shoulder since the event stating “it hurts too much”. She denies any numbness or tingling. No other complaints. Last PO intake approximately 6 hours ago. physical examGeneral: adolescent female sitting upright in bed with left arm flexed and adducted, moderate distress LUE: left arm held flexed and adducted against her body. Square-like appearance to the shoulder compared to the right which appears rounded. No erythema, abrasions, lacerations, or ecchymosis. Unable to flex, extend, or abduct left shoulder due to pain. Full flexion and extension of elbow and wrist. She can make thumbs up, okay sign, cross fingers, touch thumb to pinky, and keep fingers spread against resistance. Sensation intact in the median, ulnar and radial nerve distributions. Sensation intact in the axillary nerve distribution. 2+ radial pulse radiograph diagnosis and treatmentAnterior left shoulder dislocation. She was given intranasal fentanyl, intraarticular lidocaine and nitrous oxide. Left shoulder was then reduced by external rotation with elbow at patient’s side. No complications. Post reduction films obtained show successful reduction with no fractures discussionAnterior shoulder dislocations are the most common shoulder dislocation, accounting for approximately 95%. Majority of these occur in patients younger than 30 years old. Posterior dislocations account for about 5%, and inferior dislocations (luxation erecta) are extremely rare. Anterior shoulder dislocations occur secondary to a “hyper” external rotation. The glenoid dislocates to the position of either subcoracoid (90%), subclavicular, or sublenoid. Usually the patient holds arms by their side. In a thin patient, the acromion appears prominent giving the classic “squared off” appearance the shoulder. In larger patients, the effected shoulder may appear more round instead of its normal square shape. Intra-articular lidocaine can be used for pain relief prior to reduction as shown below.  Nitrous oxide is also a common and effective means for pain relief. A full neurovascular exam is crucial, approximately 13.5% will have neurologic injury. Axillary nerve is the most commonly effected. This nerve is tested by assessing pinprick sensation over the lateral aspect of the arm. You can also test by motor abduction of the deltoid. Films must be obtained prior to reduction if: first time dislocation, age over 40, presence of humeral ecchymosis, or traumatic mechanism. The scapular Y view will demonstrate anterior dislocation of the humeral head from the glenoid. Associated injuries to look for include Hill sachs defect, bankart lesions, fractures of the greater tuberosity, soft tissue injuries, and rotator cuff tears. While we will not discuss in depth associated injuries, it is important to be aware particularly of hill sachs and rotator cuff tears. Hill sachs defect presents in up to 40% of anterior dislocations; this defined by a radiographic defect in the posterior lateral portion of the humeral head. Rotator cuff tears, also common, present more commonly in older patients. It is estimated between 35-86% of anterior dislocations in patients over 40 years old have a rotator cuff tear. Shown below includes image of anterior shoulder dislocation with hill-sachs deformity on the left; and anterior shoulder dislocation with bankart lesion on the right. 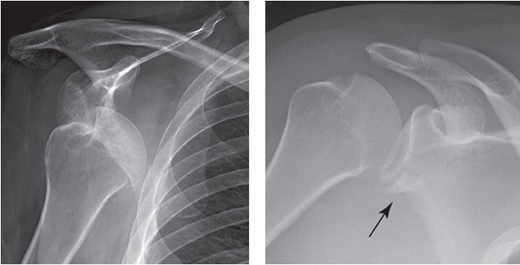 There are several techniques for reduction, none of which have proven more efficient or effective over the other. A common technique, used in this patient, is the external rotation method. Patient sits up, straight back. Examiner holds the elbow at the patients side and with forearm in 90 degree angle, slowly externally rotates the arm. After successfully reduction, the arm is immobilized with splint and post reduction films obtained. Immobilization should be for 3 weeks if younger than 30 yrs old, and for 7-10 days if over 30 yrs old.
1 Comment
HPIThis is a 13 yr old Caucasian male with no significant past medical history who is presenting with 2 week history of right hip pain. He describes a vague pain localized around the right hip worsened with movement mostly flexion and extension of the hip. No known alleviating factors. No history of trauma, fever, chills, nausea or vomiting, recent weight loss or night sweats. No other joints involved. No family history of rheumatologic or bone disorders. physical examGeneral: Obese male, laying flat on bed in no distress. RLE: Right lower extremity is slightly externally rotated compared to left. No thigh or calf atrophy. No erythema, swelling, or warmth to touch. No abrasions, lacerations or ecchymosis. 2+ dorsalis pedis pulse. Sensation intact in all dermatomes. Full active range of motion of right hip. Passive range of motion however is significant for slight external rotation with flexion of the hip. No patellar or fibular head tenderness. Full active and passive range of motion of knee. Noted to have slight external rotation of right lower extremity with gait. GU: Normal male genitalia. No erythema, swelling, or tenderness of penis or scrotum. No urethral discharge. LLE: No erythema, swelling, or warmth to touch. No abrasions, lacerations or ecchymosis. 2+ dorsalis pedis pulse. Sensation intact in all dermatomes. Full active and passive range of motion of hip. No patellar or fibular head tenderness. Full active and passive range of motion of knee. radiographs Diagnosis and treatmentIsolated right slipped capital femoral epiphysis. No involvement of the left side. Patient was taken to the operating room the following day and underwent percutaneous in situ fixation with two cannulated screws. TSH and free T4 obtained, normal. Counseling on weight loss provided. discussionSlipped capital femoral epiphysis (SCFE) is a disorder where the femoral epiphysis displaces from the femoral neck through the physeal plate. It is a common hip disorder in adolescents affecting approximately 10 per 100,000. Note however, about 15% will present with no description of hip pain but rather knee or thigh discomfort. Thus it is important to maintain a high degree of suspicion to diagnose and treat early. SCFE is more commonly seen in obese children; obesity is the single greatest risk factor. It more commonly affects males, African Americans, and Pacific islanders. Often it occurs during periods of rapid growth (the average age for boys 13 yrs old, females 12 yrs old). It can be associated with endocrine disorders including hypothyroidism, osteodystrophy of chronic renal failure and growth hormone treatment. If SCFE is diagnosed in a child who is <10 yrs old or whose weight is <50th percentile, an endocrine workup is warranted. The displacement of the epiphysis occurs secondary to mechanical forces. Through the hypertrophic zone of the physis, slippage can occur. Cartilage within the perichondral ring acts as a weak point and with mechanical forces causes displacement. With displacement, the epiphysis remains within the acetabulum. The neck slips anteriorly and rotates externally. The most common presenting complains are pain and altered gait. Classically, an obese child presents with dull pain either in the hip, groin, thigh or knee without any history of trauma. Symptoms can be present anywhere from week to several months. Often an abnormal coxalgic gait is noted. The child may have decreased hip motion with obligatory external rotation during passive flexion of the hip. There may also be abnormal leg alignment with the foot slightly externally rotated and thigh atrophy. Diagnosis is made by radiographs. It is recommended that both an AP and frog-leg lateral of the right and left hip is obtained. 17-50% of SCFE are bilateral. On the AP pelvis, Klein’s line can be drawn to help diagnose. This line is drawn along the superior border of the femoral neck. In a normal hip, the line will intersect the femoral head. In SCFE, Klein’s line does not intersect the femoral head. 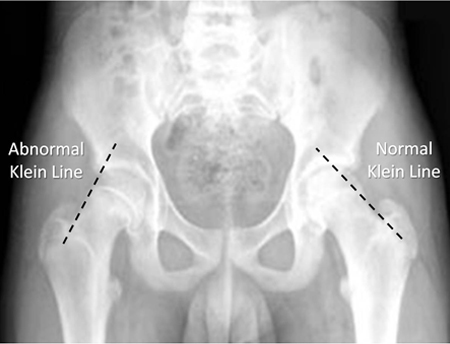 PIf the child is able to ambulate, it is termed stable. Unstable SCFE occur in children unable to ambulate or if the epiphysis is displaced from the metaphysis. Each is treated by making the child non-weightbearing until orthopedic consultation and treatment. The importance in the difference is children with unstable SCFE may have further displacement with any manipulation; thus it is extremely important to immediately place child on stretch and instruct to not ambulate. Children with SCFE should be referred to orthopedics promptly. Non-weightbearing is required until treatment. Treatment is surgical by either percutaneous in situ fixation or open reduction with the capital realignment. pearls1. SCFE is where the femoral epiphysis displaces from the femoral neck
2. More common in obesity, males, African American, and Pacific islanders 3. Can be associated with endocrine disorders 4. Order AP and frog-leg views bilaterally to diagnose, assess Klein's line 5. Urgent orthopedic consultation for surgical treatment hpi45 year old male right hand dominant with no significant past medical history presents by EMS after low mechanism motor vehicle crash complaining of left thumb pain. States his left hand “jammed into the steering wheel” during the crash causing deformity to the left thumb. He denies any numbness or tingling but is unable to fully range due to pain. No prior left hand injuries. Non-smoker. physical examSwelling and deformity to the left thumb metacarpophalangeal joint. No abrasions, laceration or ecchymosis. 2+ radial pulse. Significantly limited flexion and extension of the left thumb at the MCP. Intact flexion and extension at the PIP. 2-point sensation intact. Good capillary refill. RadiographDorsal dislocation of the left thumb metacarpophalangeal joint  Diagnosis and planSimple metacarpophalangeal joint dislocation of the left thumb. Patient was given pain medication through an IV and a radial and median nerve block was done for anesthesia. The joint was then reduced successfully at bedside with initial attempt. Post-op exam essentially unchanged except significant improvement in flexion and extension at MCP. There did not seem to be any significant instability. Regardless patient was placed in a thumb spica splint and follow-up with hand clinic in 1 week. DiscussionDislocation of digits are common. Dorsal MCP dislocations follow hyperextension of the affected joint with rupture of the volar plate. They are classified by direction as dorsal, volar, or lateral.
Dorsal: distal digit displaced toward back of hand Volar: distal digit displaced toward palm of hand Lateral: distal digit displaced ulnar or radial direction The most frequent direction of dislocation is a dorsal displacement. Metacarpophalangeal dislocations are further classified by volar plate involvement. For MCP dislocations other than the thumb this is simple (volar plate not interposed in the joint) or complex (volar plate entrapped in the joint). For MCP dislocations of the thumb, classify as incomplete (volar plate ruptured, collateral ligament intact), simple (volar plate and collateral ligament ruptured), or complex (dislocated phalanx entrapped in intrinsic hand muscles and volar plate entrapped). Simple thumb MCP joint dislocation are in extension and reducible whereas complex dislocations are in bayonet apposition and not easily reducible. It is extremely important to obtain radiographs prior to attempting reduction to clarify whether the reduction should be attempted or referral to hand surgeon. Emergency medicine physician should reduce the dislocation once confirmed a simple dislocation without associated open joint, fracture or entrapped volar plate. hpiThis is 28-year-old female history of IV heroin abuse currently on Suboxone treatment who is coming in for 4 day history of progressively worsening right hand pain and swelling. States one week ago hit her hand on a stapler with minimal trauma. Several days later she then developed pain, swelling and redness over her fourth knuckle on her right hand. The pain has been progressively worsening unresponsive to Tylenol and Motrin. She is now unable to fully extend her fourth finger due to pain. Denies any fevers, chills, nausea, vomit, diarrhea. Her history is significant for similar infection to her left hand requiring incision and drainage approximately 6 months ago. She is right-handed. Smokes daily. Physical examExam: There is significant swelling and erythema over the right fourth digit from the metacarpal joint to the PIP. Appears "sausage-like ". The right fourth finger is held in slight flexion. Patient is unable to extend the finger fully. With passive extension of the finger patient has significant pain. Significant tenderness over the entire fourth digit. Sensation intact to light touch. Radiographs: There is no evidence of fracture dislocation. Soft tissue swelling noted over the fourth finger Laboratory data: White blood cell count 9.7, sedimentation rate 10, C-reactive protein 2.6 DIanosis/ planPresentation consistent with tenosynovitis. She was given IV antibiotics, evaluated by orthopedics at bedside. Taken to OR for I&D. DIscussionTenosynovitis is an inflammation of a tendon and it is synovial sheath. It most frequently occurs in the hands and wrists however can occur in any joint. Tendon sheaths have 2 surfaces, a visceral layer (inner) and a parietal layer (outer). When fluid and inflammatory markers accumulate between these two layers and their potential space, this is referred to as tenosynovitis. There are 3 mechanisms that accounts for most episodes of tenosynovitis: 1. Trauma (puncture wound, laceration) 2. Contiguous spread from adjacent infected soft tissue 3. Hematogenous Organisms: The most common pathogens are skin flora including Staphylococcus aureus and Streptococci. However, any organism can cause tenosynovitis. Tenosynovitis is a clinical diagnosis. There are four classic clinical findings as described by Kanavel: Tenderness over the entire flexor tendon sheath, symmetric finger swelling over the length of tendon sheath described as "sausage-digit", intense pain with passive extension, resting flexed posture of digit to minimize pain. Often radiographs are obtained to rule out fracture or bony involvement. Often these are normal. No lab tests are sensitive or specific to tenosynovitis. pearlsTenosynovitis is a clinical diagnosis
Recognize Kanavels four classic clinical findings Broad spectrum antibiotics HPI:
The patient is a 41-year-old female with past medical history of diabetes who presents with right knee pain. Patient states that approximately 2 days ago, she noticed that her knee was red, swollen, and has gotten sore to the point that she cannot walk. Patient denies ever having symptoms like this before. Patient denies any prior surgeries or trauma to the joint. Physical exam: Swelling and erythema over the right knee. The patient is unwilling to walk in the exam room stating that she cannot secondary to pain. The knee is warm to the touch with no overlying induration. The patient has limited active and passive range of motion secondary to pain. Patient has 2+ distal pulses with intact sensation to light touch in all dermatomes. Radiographs: Normal knee Laboratory data: CBC: WBC 24K, Platelets 224 Serum glucose: 197 ESR: 39 CRP: 7.2 Joint aspiration: cloudy fluid, WBC 62K, gram stain negative, glucose 94 Diagnosis and Plan: Septic arthritis. Patient was started on vancomycin and orthopedics was consulted. She was admitted to the hospital and taken to the OR later that night for washout. Discussion: Location: The most commonly affected joints in descending order are the knee (>50%), hip, shoulder, elbow, ankle, sternoclavicular joint. Risk Factors: Greater than 80 years of age, presence of prosthetic joint, overlying skin infection, diabetes, rheumatoid arthritis, cirrhosis, HIV, history of gout or pseudogout, endocarditis, recent bacteremia, IV drug user, recent joint surgery. Organisms: Most common in all patients is Staphylococcus aureus which accounts for greater that 50% of infections. There are some specific patients that have high rates of other organisms that we should be aware:
ER Work-up:
Differential: An emergency physician is only as good as the differential that they consider, therefore, we should maintain the following on their differential: gout, pseudogout, reactive arthritis, rheumatoid arthritis, Lyme disease, gonococcal arthritis, traumatic arthritis, cellulitis, bursitis. Treatment: There are no good randomized controlled trials for antibiotic treatment of septic arthritis. Current recommendations are based on the most likely organism. If you lucky enough to have a positive Gram stain, then you should treat gram-positive smear with vancomycin and gram negative smear with a third generation cephalosporin such as ceftriaxone. Other specialized considerations are:
Finally, once confirmed, orthopedic service should be consulted as these joints will need washout in the operating room. Pearls:
|
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
