|
HPI: The patient is a middle-aged male with PMH of diabetes and hyperlipidemia who presented to the emergency department with right second toe pain. Two months prior, the patient dropped a heavy object on his toe causing the nail to fall off. Since that time, he has had persistent pain in that digit. Seven days prior admission, the patient reports that his second right digit turned black with associated right foot swelling and erythema. Patient denied any systemic symptoms. PE: Right second toe is black and entirely discolored with obvious necrosis. Minimal peeling at the plantar surface, 2+ DP and PT pulses bilaterally. Decreased sensation over the 2nd right toe. Patient is able to flex and extend all digits without difficulty. Mild erythema over the dorsum of the foot.  Imaging: Right foot xray: Peripheral calcified vasculopathy concerning for ischemic change. Negative for tissue pneumatosis. Negative for stress fracture. Mild degenerative arthrosis of the talonavicular joint. CTA Pelvis with unilateral runoff: Diffuse scattered atherosclerotic and intimal thickening changes within the patient's right lower extremity. Runoff from the superficial femoral artery to the level the popliteal artery. There is severe diffuse atherosclerotic change of the posterior tibial artery extending to the plantar aspect of the foot and also to the vessels supplying the digits.  Management:
Patient received IV antibiotics in the ED given the erythema over the plantar surface of the foot. Patient admitted to orthopedic service and underwent amputation of 2nd digit. Discussion: -Gangrene is the progressive death of tissue secondary to lack of blood supply -Two most common types are dry and wet -Dry gangrene is secondary to lack of blood supply. Wet occurs when tissue becomes infected with bacteria. -Patients are increased risk because of conditions such as diabetes, trauma, smoking, obesity, excessive alcohol use and IV drug use -Symptoms include pain, shedding of skin, foul smell and skin color changes. Systemic symptoms include fever, chills, confusion, nausea, vomiting, diarrhea, and hypotension -Diagnosis includes basic laboratory work-up, xray of the affected area, CTA as needed -Treatment includes IV antibiotics to treat any overlying infection, supportive care including fluids and pain control, surgical debridement, revascularization if possible, hyperbaric oxygen and amputation if all else fails Key Points: -Initiate antibiotics early if infection is suspected -If ischemia is detected early, revascularization with vascular surgery consultation is recommended -Dry gangrene is a result of chronic ischemia -Once gangrene has developed, affected tissue is typically not salvageable and orthopedics or vascular surgery should be consulted by amputation -Gas gangrene is caused by exotoxin producing bacteria and should always be on an emergency physicians differential – ALWAYS consider this on the differential
0 Comments
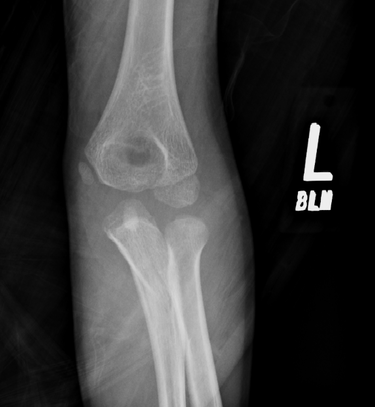
HPI: Young male otherwise healthy presenting today status post fall. Right hand dominant. Patient fell awkwardly with his arm slightly outstretched backwards off a trampoline and landed with his left arm under him. Patient had isolated pain at his left elbow. Ambulatory. No head injury or LOC. Physical Exam: Mild swelling present at the left elbow region with tenderness at the olecranon. Patient had limited range of motion at the elbow secondary to pain. Radial pulses strong and equal bilaterally. Able to give thumbs up, cross fingers, and make okay signs bilaterally. No neurologic deficits in median, radial or ulnar nerve distributions. Radiograph:
Management:
HPI:
33 year old with no prior PMH presents to the ED with left knee pain Physical Exam: Swelling over the left knee. Limited range of motion secondary to pain. No overlying laceration or abrasion. Knee is warm to the touch. Overlying cellulitis on the lateral left knee. Palpable DP and PT pulses with intact sensation in the SP, DP and tibial nerve distributions. Radiology: Normal knee Management: Patient underwent arthrocentesis. Joint fluid analysis showed only 81 cells. Presentation consistent with cellulitis and patient improved with IV antibiotics. Discussion: -Most commonly affected joints in descending order: knee, hip, elbow, ankle, sternoclavicular joint -Joints become infected by 1) bacteremia, 2) direct inoculation 3) contiguous spread from adjacent osteomyelitis -Why does it matter? It causes irreversible cartilage destruction in the joint -Involved joint is tender, warm and erythematous -WBC count, ESR and CRP aid in the diagnosis -Diagnosis is by joint fluid analysis – TAP THE JOINT! -Treatment includes early antibiotic treatment and operative irrigation and drainage of the joint Key Points: -Always think of this diagnosis when a patient presents with a tender, warm and erythematous joint -Diagnosis is by joint fluid analysis – TAP THE JOINT! -THIS IS AN ORTHOPEDIC SURGICAL EMERGENCY – Involve consultants early! HPI: Middle aged female presents with right foot pain after "twisting" her foot. Physical Exam: Swelling present over the dorsum of the foot. No overlying laceration or abrasions. Palpable DP and PT pulses with intact sensation in SP, DP and tibial nerve distributions. Tenderness present over the base of the 2nd metatarsal. Unable to bear weight on RLE. Radiology: demonstrates oblique fracture at the base of the 2nd metatarsal  Management:
We placed the patient in a well padded posterior leg splint and patient was instructed to not weight bear on her RLE. She was given follow up with orthopedics in 10 days for re-evaluation once swelling improves. Discussion:
HPI:
Middle age male with no significant PMH presents to the ED after amputating his right index distal fingertip. Physical Examination: Patient has a right transverse (slightly volar oblique) index fingertip amputation with distal tuft visible within the wound. The laceration grazed the nailbed. Sensation is intact in the radial/medial/ulnar distributions of the hand including throughout the index finger. Radial pulse is palpable and the finger has good capillary refill. Radiology: XR of right hand is notable for distal tuft amputation but negative for foreign body. Management: Approximately 1mm of the nail plate was removed exposing the edge of the nailbed. Soft tissues, including the fat volarly and the nailbed dorsally were elevated off of the distal phalanx. Distal phalanx was then rongeured until sufficient soft tissue could be mobilized to cover the bone. The soft tissue was then sutured close. The wound was covered with Xeroform and dressed. Ancef was given prior to discharge. Orthopedic follow up was arranged for the following day. Discussion:
|
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|

 RSS Feed
RSS Feed
