|
HPI: young male s/p ATV accident Exam: Inspection: edema and deformity. No open wounds. Palpation: TTP, palpable deformity. 2+ DP/PT pulses. SILT lower extremity. ROM: unable to perform straight leg raise. limited ROM secondary to pain. Limited assessment of anterior/posterior drawer, varus/valgus testing Imaging: # Best seen on lateral xray. #In pediatric patients, MRI if xrays do not show fracture and child unable to perform straight leg raise   orthobullets.com orthobullets.com Bipartate patella: #often mistaken for fracture-use history and clinical exam #8-10 % of population, 50 % bilateral, usually superolateral Fracture Patterns:
Management: # Nonoperative: -Extensor mechanism intact (straight leg test) -nondisplaced/minimally displaced -vertical fractures -Knee immobilized in extension (cylinder cast/brace) #Operative -extensor mechanism failure -open fractures -articular displacement > 2 mm -displacement > 3 mm -patella sleeve fractures in children (fracture between cartilage sleeve and patella) -severely communited fractures Discussion: -Patella fractures 1 % of skeletal injuries -Mechanism: direct impact of indirect eccentric contraction -Complications: weakness and anterior knee pain, loss of reduction, nonunion, osteonecrosis, infection, stiffness Key Points: #History of mechanism and exam is important-especially palpation, straight leg testing #Best seen on lateral xray, consider MRI in pediatric patients given history and exam findings #Bipartate patella-seen in 8-10 % of population, usually superolateral #Orthopedic consultation-open vs closed, fracture pattern, straight leg testing, displacement #Consider patella sleeve fractures in pediatric patients #Management-minimally displaced, vertical, closed, extensor mechanism intact-immobilize in brace or cast and follow up as outpatient; Open, extensor mechanism not intact, communited, displaced-surgical
0 Comments
HPI: Toddler with history of osteogenesis imperfecta type 1 presented after a fall resulting in bruising to right lower extremity, fussiness. Exam: vs normal 5 cm bruise to mid right shin, 2+ DP/PT pulses, cap refill < 2 sec. Full range of motion at hip, knee and ankle joint. Intact plantar, dorsiflexion, leg extension. NO laxity or pain with valgus or varus stress testing. Imaging: -Require AP and lateral views of tibia and fibula, ipsilateral knee and ankle -Imaging below shows a non-displaced spiral tibial shaft fracture  Management:
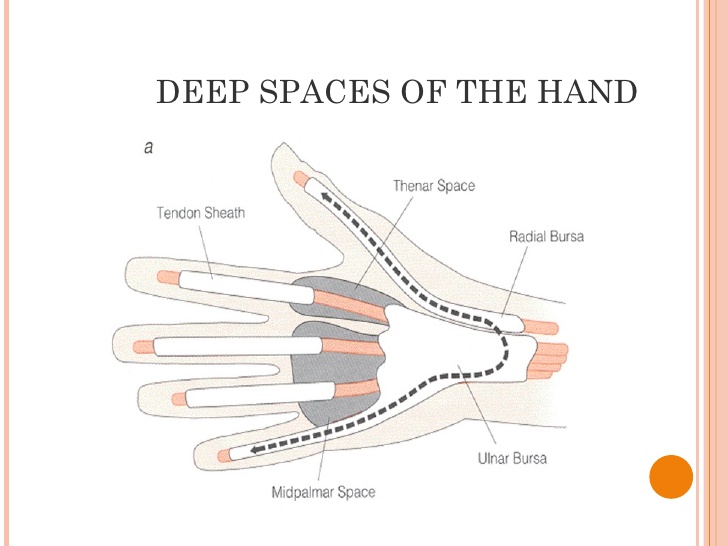
-Closed reduction with long leg cast -Follow up with orthopedics in 2 weeks Anatomy: -Distal half of tibia, fibula usually remains intact Discussion: -15 % of all pediatric fractures -If not walking yet, consider NAT -May present with bruising, limping, refusal to bear weight -Mechanism usually low energy with rotation Key Points: -Toddler fractures common (15 %) -Consider NAT if not walking yet -AKA childhood accidental spiral tibia (CAST) fractures -MOI: low energy, rotation -History: pain, limp, not bearing weight -Exam: warmth, pain, bruising, pain with ankle dorsiflexion -Obtain: xrays AP/lateral tibia/fibula, ipsilateral knee and ankle -Manage with closed reduction and long leg cast with orthopedic follow up in 2 weeks -Prognosis: good, usually heal in 3-4 weeks -Complications: compartment syndrome, leg-length discrepancy, angular deformity HPI: Teenage RHD healthy male presented initially to PCP with blister to left hand from playing baseball. Small blister incised and culture sent which eventually grew out MRSA and he was started on bactrim. On follow up 4 days later swelling worsened with worsening surrounding erythema. Denied fevers ,chills or other symptoms. Denied insect, spider or other exposures. Admitted for IV antibiotics and ortho hand consultation. Exam: afebrile, vitals normal 2+ radial pulse, cap refill < 2 sec SILT throughout hand and digits Flexion/Extension/adduction/abduction intact and notable only for mild pain with flexion of thumb, area of fluctuance to radial aspect of palm extending from mid palm around to dosal aspect of 1st and 2nd digits; see picture
Imaging:
Management: Orthopedic hand consultation Admission for IV antibiotics
Anatomy: 3 main deep spaces: potential spaces separated by fascial septum
Key Points:
By: Dr Bryon Callahan
|
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|



 RSS Feed
RSS Feed
