|
HPI: 22 yo otherwise healthy male presents s/p head on MVC vs tree. Patient is awake and alert, hemodynamically stable, complaining of right hip pain. Physical Exam: No external signs of trauma. Right lower extremity is shortened compared to the left and internal rotated. No numbness, 2+ DP pulse.   Classification: - Simple: pure dislocation - Complex: with associated fracture of acetabulum or proximal femur Mechanism: - Axial load on femur while hip flexed and adducted or through flexed knee (dashboard injury such as this patient) Requires emergent reduction (within 6 hours!) due to risk of vascular compromise to hip and osteonecrosis However... Examine femoral neck closely on XR to rule out fracture prior to attempting closed reduction. With ipsilateral femoral neck fracture, closed reduction is contraindicated! 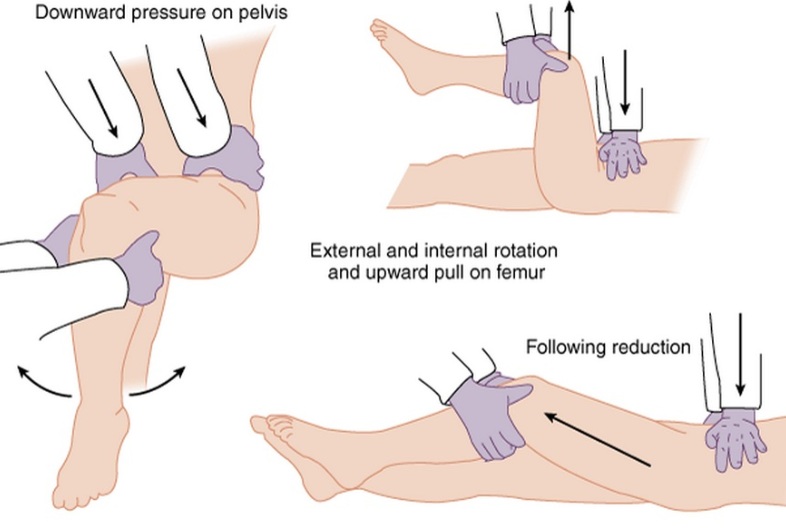 Patient must be adequately sedated for procedure. Propofol helps with tissue relaxation! Post reduction CT must be performed to evaluate for: - femoral head fractures - loose bodies - acetabular fractures Commonly associated with ipsilateral knee injuries (up to 25%) Dispo: For simple dislocation, protected weight bearing for 4-6 weeks Resources: 1. Serna, Fernando MD, Corczyca, John MD. Hip Dislocations and Femoral Head Fractures. University of Rochester Medical Center. March 2004. 2. Orthobullets.com
1 Comment
Your comment will be posted after it is approved.
Leave a Reply. |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
