|
HPI: 5 year old female presents with right arm pain after falling on a chair. Her arm was pinned in between the chair and the floor. She had immediate pain but it resolved. The following day she has increased pain and swelling in the right arm. EXAM: Swelling is noted in the proximal forearm. Tenderness to palpation present on the proximal ulna as well as radial head. No tenderness to the medial condyle, lateral condyle, or olecranon. Passive and active range of motion of the elbow is full but painful. No motor or sensory deficits of the hand. IMAGING. AP and lateral views of the elbow.   Note there is plastic deformation of the ulna without a complete fracture
Always assess the radial head, it should point towards the capitulum MANAGEMENT #Non-operative - Closed reduction of ulna and radial head dislocation and long arm casting - If no ortho available, attempt to reduce radial head and place in a posterior splint. - Axial traction traction to restore ulnar length - Need to successfully reduce radial head dislocation as well - Immobilize in 110 degrees flexion and full supination. #Operative - Indicated if radial head or ulnar length are unstable following reduction - Indicated in Bado Type IV fractures (complete fx of Ulna and Radius) - Frequently required in missed diagnosis. DISCUSSION - A Monteggia fracture is radial head dislocation plus a proximal ulna fracture or plastic deformation of the ulna - Peak age range 4-10 years, fall onto pronated arm.. - Frequently missed since the ulna may only have plastic deformation, have a high suspicion if there is pain over the radial head or evidence of radial head dislocation. - Complications include posterior interosseous nerve neurapraxia (finger drop, radial wrist deviation). - Loss of forearm motion with delayed treatment (2-3 weeks) - Different classifications are present (Bado) but not as key as recognizing the fracture. - This patient was casted and follow up arranged. KEY POINTS - Have a high index of suspicion when there is radial head tenderness or dislocation - Ulna may show only plastic deformation - Radial head should always point towards the capitulum - Obtain contralateral arm films if comparison is needed. - ED management without ortho includes reduction with posterior splint placement. Close f/u. - Majority of cases result in non-operative management. - Frequently missed By Dr. Mohamed El-Kara REFERENCES http://www.orthobullets.com/pediatrics/4015/monteggia-fracture--pediatric http://emedicine.medscape.com/article/415822-overview#a5
0 Comments
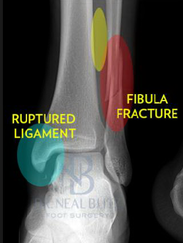
HPI: Middle age male who presents with left ankle pain, swelling, and deformity s/p fall down stairs. Unable to bear weight to LLE. Physical Exam: obvious deformity, edema, ecchymosis to L ankle. TTP over medial and lateral malleolus. Unable to flex and extend at ankle 2/2 pain. DP/PT 2+. Normal sensation to light touch to dorsal surface/plantar surface/1st web space. IMAGING:
Diagnosis and Management: This patient has a Weber B distal fibula fracture with medial subluxation of the tibia and disruption of the mortise joint. Combination of distal fibula fracture and likely complete disruption of deltoid ligament is a bimalleolar fracture-dislocation equivalent. Thus, this is an UNSTABLE ANKLE! Patient’s ankle was reduced using axial traction and inversion, placed in posterior sugar tong splint. Injury required 3 reductions, which is common due to the instability of this injury. Patient was admitted to Orthopedic Trauma service and scheduled for next day ORIF.
HPI: Middle-aged male s/p MCC. PE: Ecchymoses, swelling, and tenderness about ankle. Tender over proximal fibula and pain with squeezing of calf. Figure 1: Mortise view of ankle showing widened mortise medially Figure 2: Leg film showing proximal fibular fracture Ankle Sprains: - Divided into grades o I: Minor, no significant ligamentous damage. Able to bear weight. o II: Associated with partial ligamentous tear. Significant ecchymoses/swelling. Difficulty bearing weight. o III: Associated with complete ligamentous tear. Significant functional loss and universal inability to bear weight. - When should we obtain radiographs?: o If pretest clinical suspicion is high based on mechanism of injury or patient cannot be ruled out for fracture based on Ottawa ankle rules: 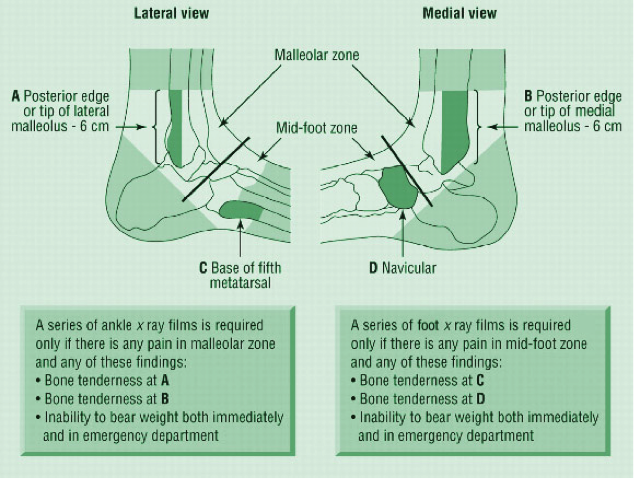 Syndesmotic injuries (AKA “high” ankle sprains):
o PE and mechanism:
o Treatment:
- Otherwise patient needs syndesmotic screw fixation. Patient can be immobilized and follow-up as an outpatient for surgical fixation HPI: Patient presents with a grossly deformed right upper extremity. PE: Gross deformity of humerus, no open fracture. Unable to extend wrist. Unable to hyper-extend MP joints of fingers and unable to flex IP joint of thumb. Radial and ulnar pulses intact. IMAGING: Multi-factorial fracture along the mid third of humerus along the expected course of the radial nerve. DISPO (if at free standing ED): Transfer patient to ED with on-call orthopedics for definitive fixation. Reduce and splint prior to transfer. TREATMENT: Nonoperative managment. Splinted and cast at bedside. Follow radial nerve palsy clinically for improvement.  |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|



 RSS Feed
RSS Feed
