|
HPI: Pediatric male presents after a fall onto outstretched arm with obvious deformity to right elbow. PE: Patient is unable to cross fingers and has paresthesias in the ulnar nerve distribution. Initial radiograph showed posterior dislocation with questionable hyperdensity representing the medial epicondyle. We were unable to reduce under fluoroscopy as the medial epicondyle was more visible and the patient eventually required ORIF. Imaging: AP and lateral radiograph of the elbow 
Image 1: Showing associated medial epicondyle fracture How to Diagnosis: Two important lines help in making the diagnosis; radiocapitella and anterior humeral. Radiocapitellar line: Drawn through the center of the radial neck and should pass the center of the capitellum as shown below 
Anterior humeral line: Drawn through the lateral view of the surface of the humerus and should pass through the middle of the capitellum 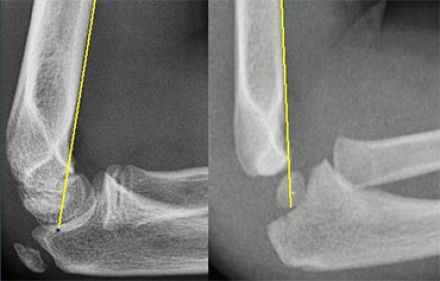
Ossification: 6 sites that fuse at different ages. Mnemonic = CRITOE
Treatment: Nonoperative with closed reduction and early range of motion (1-2 weeks) is most common. ORIF required for incarcerated medial epicondyle, inability to obtain close reduction, or significant instability. Pearls:
0 Comments
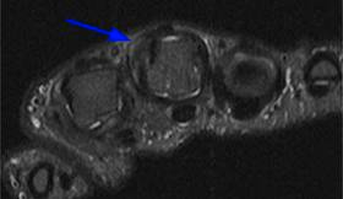
HPI: Young male presents after feeling a pop in his finger after he dropped a case of bottled water causing his middle finger to get caught in the wrapping. PE: Ulnar deviation of affected digit and a popping sensation and pain when flexing his fingers.
Imaging:
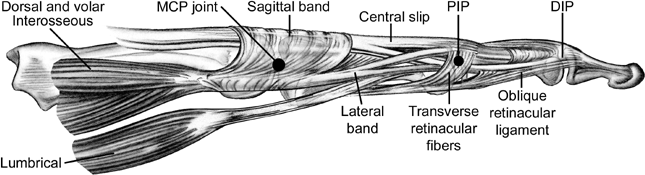
Anatomy:
Treatment Options:
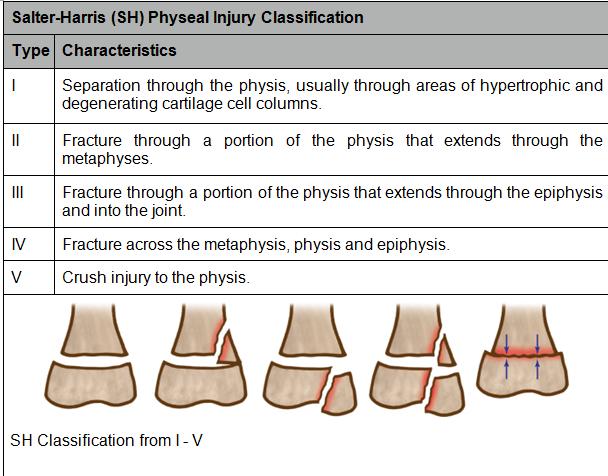
Case: 13 y/o obese AA male presents with left leg pain after stepping in a hole during football training with his brothers. States he felt a pop during this incident and has since been unable to move his leg secondary to pain. Physical exam notable for normal vital signs, edema and tenderness to palpation proximal to left knee. Sensation intact to light touch throughout, 2+ pulses, 5/5 strength of ankle/great toe dorsi/plantar flexion. Diagnosis: Plain films including 2 view femur, 3 view knee, and 2 view tibia/fibula MRI (now gold standard) or ultrasound when plain films not diagnostic and suspicion still high 
 Case: 27 year old Male s/p MVC with multiple open RLE fractures. Complains of severe pain at the BL ankles, unwilling to allow any further testing in the trauma bay. Plain films of single ankle below: 
 Calcaneal Fractures: - Mechanism: Generally result from an axial load to the lower extremity. Typically either a fall from height while landing on one’s feet –or- from an MVC. - Presentation: Patients may have a shortened and widened heel with varus deformity. Patients also may have “Mondor’s sign” which is ecchymoses of the foot extending into the heel. Diagnosis:

CT Scans:
Classification: There are multiple levels of classification, but the most important delineation is between intra-articular and extra-articular fractures.

As stated before -> Calcaneal fractures are associated with significant axial load so always consider other injuries including hip/pelvis, or lumbar spine fractures.
Treatment: o For most extra-articular and type I intra-articular fractures: Immobilization with short-leg splint, strict non weight-bearing status, elevation, pain control. Patient will need ortho follow-up ASAP. o For more severe fractures: Surgical fixation, if pursued, will vary depending on the patient’s comorbidities and the preference of the surgeon. Important complications: o Poor wound healing (particularly in smokers and diabetics) o Compartment syndrome o Arthritis |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|

 RSS Feed
RSS Feed
