|
HPI: Right hand dominant middle aged female with history of HTN presents to the ED after accidentally hitting her left index finger with a hammer while working on a home improvement project. Finger is painful and swollen but she has no other injuries and reports she is otherwise feeling well. Physical Examination: Erythematous, swollen, and tender left 2nd distal phalanx. There is a subungual hematoma present over approx. 75% of the nail but the nail is intact. Motor and sensation intact, full ROM of PIP and DIP, 2+ radial pulse, no other injuries identified. Radiology: AP, lateral and oblique views of left 2nd phalanx – no fracture or dislocation identified Management: Nail removal and bedside repair of nail bed laceration, tetanus updated, discharged home with 48 hour follow up for reevaluation Discussion: Fingertip injuries = most common hand injuries seen in the ED Most common mechanisms:
Evaluate for:
Complications of injury:
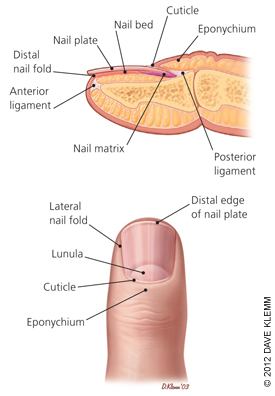 Image obtained from Am Fam Physician. 2012 Apr 15;85(8):779-787. Fingertip Anatomy:
Blood Supply and Innervation:
Nail Growth:
Treatment: Obtain radiographs to rule out distal phalanx fracture Evaluate for subunginal hematoma and nail bed lacerations Drain hematoma if <50% nail involved
Nail removal, I&D, repair of nail bed if >50% of nail involved
0 Comments
HPI: 20ish year old and otherwise healthy male presents as the restrained driver in head-on MVC at low speed just prior to arrival. He has a large linear laceration to anterior aspect of R knee and is unable to fully extend the knee. Wound is hemostatic. No other injuries or complaints. Physical Examination: 10cm linear, horizontal laceration to the anterior aspect of the patient’s R knee. Knee is held in slightly flexed positioning. Decreased ROM of the knee secondary to pain and injury, patient unable to actively extend extremity in straight leg raise. FROM of ankle. 2+ DP and PT pulses present. Sensation intact to light touch throughout. No erythema, swelling or significant tenderness present over RLE. Radiology: AP/Lateral/Sunrise/Oblique views of R knee: Transverse fracture of the patella with 3mm of displacement present and surrounding soft tissue edema Management:
Discussion:
Types of fracture:  Figure obtained from jaaos.org; Patellar Fractures in Adults; AAOS April 2011 vol. 19 no. 4 198-207,Figure 4 A) Nondisplaced B) Transverse C) Pole or sleeve (upper or lower) D) Comminuted nondisplaced E) Comminuted displaced F) Vertical G) Osteochondral Evaluate with physical examination first Severe knee pain and soft tissue swelling should raise suspicion for injury Concerning findings:
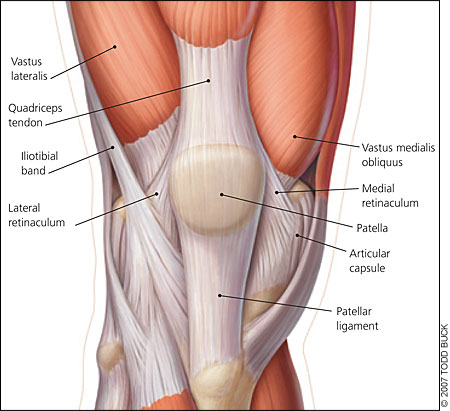 Image obtained from aafp.org, Am Fam Physician. 2007 Jan 15;75(2):194-202. Obtain Radiographs
Fracture displacement best viewed on lateral films, but obtain AP/Lat/Oblique/Sunrise to fully evaluate Degree of displacement = degree of retinacular disruption Treatment: Nonoperative:
Early active ROM with hinged knee brace after 2-3 weeks Operative:
Pearls: Watch out for patella sleeve fractures in peds – need high index of suspicion to diagnose
Bipartite patella = failure of bony fusion
Any lacerations present must be assumed to communicate with the knee joint until this assumption is disproved by a saline load joint challenge A patellar fracture is problematic and requires intervention if extensor mechanism of knee is nonfunctional = unable to perform straight leg raise test HPI:
Pre-teen male with no PMH presents to the ED after a dog bite the night before. Patient was bit on the palm of his left hand by a relative’s pit bull known to be fully vaccinated. Wound had been becoming more painful and 3rd digit is more swollen, painful, and difficult to range. No other injuries or complaints. Physical Exam: Two sub-centimeter puncture wounds to the center of the palm of the left hand, hemostatic with small amount of surrounding erythema present. 3rd digit with fusiform soft tissue swelling, increased warmth, and significant tenderness to palpation. Finger in slightly flexed positioning. Decreased ROM of the 3rd digit with flexion and significant pain with passive extension. Sensation intact to light touch throughout digits and hand. No other erythema, swelling, or significant tenderness present over LUE. 2+ palpable radial and ulnar pulses present. Radiology: No fracture or acute changes. No foreign body present. Management: Patient was admitted and was started on IV antibiotics for suspected pyogenic flexor tenosynovitis. Wound was rechecked in the morning with minimal improvement in symptoms and patient underwent I&D of digit and hand with continued IV antibiotics. Discussion: Pyogenic flexor tenosynovitis = infection of synovial sheath surrounding the flexor tendon
Pain/swelling usually delayed 24-48 hours, usually localized to the palmar aspect of one digit of the hand Kanavel signs – key physical exam findings for diagnosis
Obtain x-rays to rule out bony involvement or foreign body MRI can help diagnose but is expensive and generally unnecessary since clinical exam usually is sufficient Treatment: If early presentation:
If late presentation or if no improvement after 24 hours of conservative treatment:
Empiric Abx to consider: Otherwise healthy individuals--
Consider with dog bites-- most are polymicrobial:
Key Points: History and physical examination is key to diagnosis Start antibiotics early Consider surgical intervention when there is:
o flexor tendon sheath o deep spaces of the palm o joint spaces Kanavel signs may not be seen if patient has:
|
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
