|
HPI: Otherwise healthy middle-aged male presents to ED with L hand pain. He is a painter, and while cleaning a high-pressure pneumatic pain gun it accidentally discharged into the palm of his L hand. He reports only moderate pain at the site. Denies any other injuries, all vital signs within normal limits. Event occurred 2 hours prior to ED arrival. Exam: Pin-hole size puncture wound on palmar surface of hand w/ moderate tenderness to palpation and minimal surrounding erythema. Full passive/active ROM of all digits, neuromuscular function completely intact. Cap refill <2 seconds in all 5 digits. X-ray is unremarkable.  Discussion: High-Pressure Injection Injuries occur when a high-pressure injection device (pneumatic paint gun, grease gun, diesel injector, etc) injects into the operator. Most common in male laborers in painting and automotive industries, and injury often occurs during cleaning of the device or while attempting to clear the nozzle. Non-dominant hand involved ~75% of the time, with index finger injury most common, followed by middle finger and palm. Despite benign outward appearance, there is almost always significant underlying damage, and should be considered a SURGICAL EMERGENCY. Our job as ED providers is to recognize the seriousness of the injury and involve a hand surgeon as fast as possible! Pathophysiology involves direct trauma resulting in local tissue damage, acute and chronic inflammation, and foreign body granuloma formation. Tissue ischemia/necrosis from vascular compression, chemical inflammation, and secondary infection can lead to devastating functional outcomes, including amputation. Key historical details that impact prognosis:
Time from injury to treatment is the most important prognostic factor. Delay of >10 hours significantly increases risk of amputation. Higher PSI and larger volume of injected material portend greater direct tissue damage. Hydrocarbon-based substances (fuel, organic solvents, oil-based paint, paint thinners) cause more severe inflammatory reaction and tissue necrosis, with amputation rates >50%. Grease, latex, and water-based paints re typically less destructive. Obtain plain films in the ED to rule out coexistent fracture/dislocation. Some injected materials may appear radiopaque on x-ray and could aide in pre-operative planning. Administer broad-spectrum parenteral antibiotics in the ED, and update tetanus status. Control pain as needed, and arrange for emergent orthopedic/hand surgery evaluation. Transfer to Trauma Center if necessary. Patient will need emergent operative irrigation and debridement. Patient in HPI above had excellent functional outcome due to early presentation. Below is a time-course representation of patient with a delayed presentation, outlining potential damage that can occur. 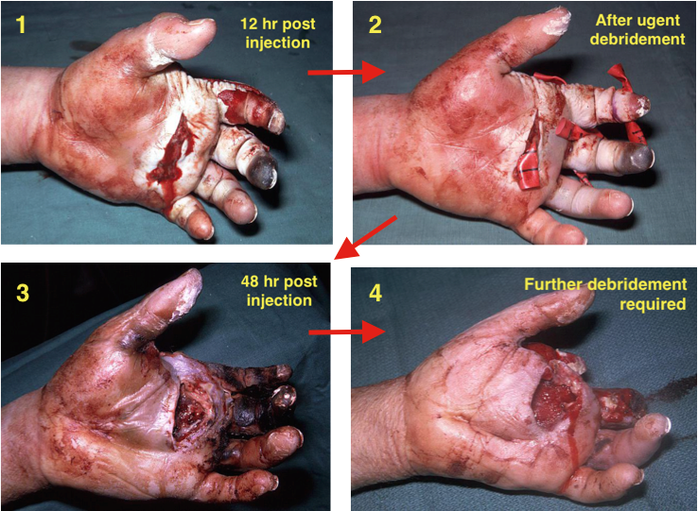 Management Pearls:
By Dr. Blake Johnson References: 1. Aiyer, A. "High-Pressure Injection Injuries." OrthoBullets, 15 Mar 2014. Web. Retrieved 25 Sept 2015, from http://www.orthobullets.com/hand/12104/high-pressure-injection-injuries. 2. Sanford, S. "High-Pressure Hand Injury." eMedicine/Medscape, 12 Nov 2013. Web. Retrieved 25 Sept 2015, from http://emedicine.medscape.com/article/826620-overview. (multiple images) 3. http://lifeinthefastlane.com/high-pressure-injection-injury/ (image)
0 Comments
HPI: Otherwise healthy middle-aged male presents to ED with L wrist pain following moderate speed motorcycle collision. There was immediate pain/swelling to L wrist, and he is reluctant to range the joint. He was helmeted and wearing full protective clothing. Denies other injuries, all vital signs within normal limits. Exam: Prominent L wrist swelling. Dorsal aspect of radial head firmly palpated beneath the skin with slight volar displacement of hand relative to forearm. Skin intact, compartments are soft. Radial and ulnar pulses palpable, distal cap refill <2 seconds. Distal motor function intact, slightly diminished sensation in median nerve distribution of L hand. (X-ray shown below) 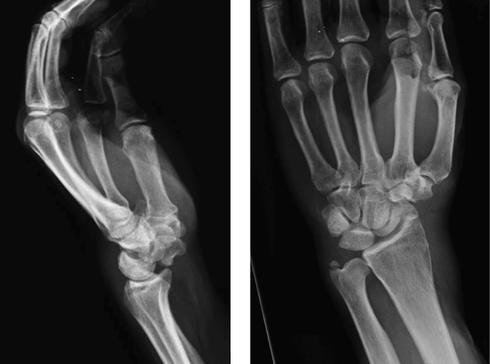 Radiologist Interpretation: Perilunate dislocation. Concomitant scaphoid waist fracture (central third) w/ distal anterior displacement. Minimally displaced ulnar styloid fracture. Discussion: Lunate dislocation (perilunate dissociation) is a high-energy injury with poor functional outcomes that almost universally requires operative intervention. Unfortunately they are commonly missed on initial presentation (~25%) due to subtleties on radiographic imaging. First, a review of normal carpal anatomy, characterized by 3 smooth lines called Gilula’s arcs: 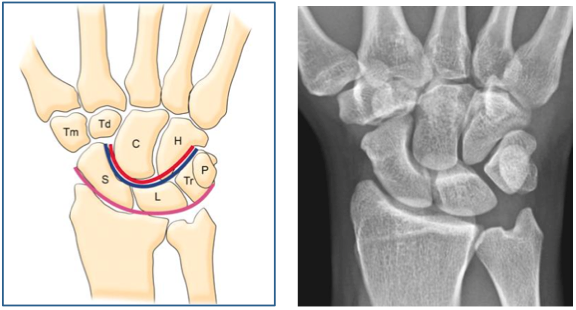 Any disruption in Gilula’s arcs raises suspicion for carpal fracture/dislocation. Lateral wrist film is essential to confirm normal in-line alignment of the radius, lunate, and capitate: 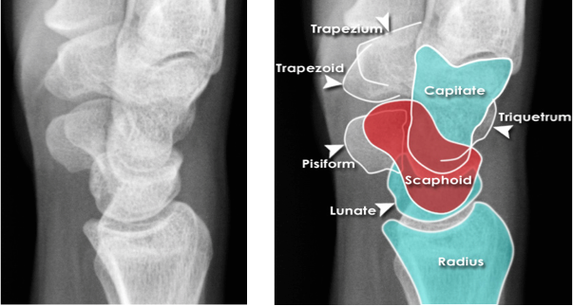 Mechanism of lunate dislocation typically involves high-energy axial load to the wrist, trapping the hand in hyperextension with ulnar deviation. Results in relative intercarpal supination causing varying degrees of carpal ligamentous rupture and articular dissociation. Injury pattern occurs in a step-wise sequence of events corresponding to Mayfield Classification System: · Stage I -> Scapho-lunate dissociation (SL widening) · Stage II -> Above w/ luno-capitate disruption (capitate overrides lunate) · Stage III -> Above w/ luno-triquetral disruption (true “perilunate dissociation”) · Stage IV -> Lunate completely dislocated from lunate fossa (usually volar, i.e. “spilled tea cup sign”) 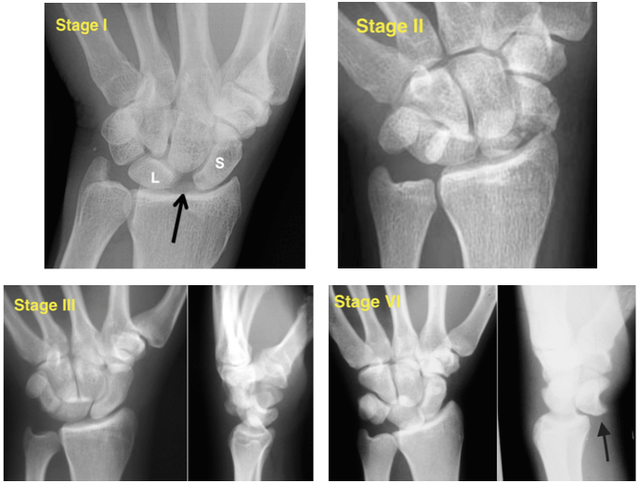 In addition to pain, stage IV dislocation and/or surrounding wrist fracture-dislocation can present with carpal tunnel compression and median nerve symptoms (~25% of patients). Emergent orthopedic consultation recommended. Closed reduction is performed in the ED using fingertraps to apply traction and to distract carpal bones while applying a sugar tong splint (may be all that is necessary). For complete lunate dislocations (stage IV), lunate must be relocated back into lunate fossa: 1) Apply gentle traction w/ wrist slightly extended 2) Manual pressure to palmar projection of lunate while flexing wrist until “snap” occurs (indicates relocation as proximal pole of capitate overcomes dorsal lip of the lunate) 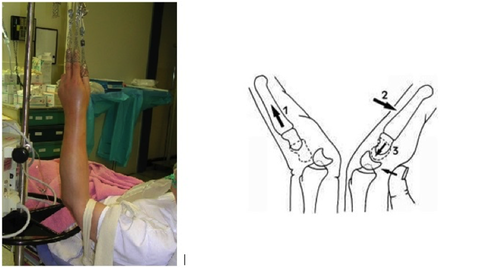 All acute lunate/perilunate dislocations require operative treatment with ORIF, ligament repair, and possible carpal tunnel release. There is universally poor functional outcomes with non-operative treatment, and recurrent dislocation is the rule, not the exception.
Management Pearls: · Know radiographic pathoanatomy, EASY TO MISS! · Assess for median nerve pathology and vascular injury · Emergent orthopedic consultation · Closed reduction with finger traps, apply sugar tong splint · Likely does not require admission, but operative treatment ASAP · High energy mechanism, don’t miss coexistent fracture or other injuries By Dr. Blake Johnson References: 1. Karadsheh, M. “Lunate Dislocation (Perilunate Dissociation).” OrthoBullets, 24 Dec 2014. Web. Retrieved 16 Sept 2015, from http://www.orthobullets.com/hand/6045/lunate-dislocation-perilunate-dissociation. (multiple images) 2. Murray, P. “Perilunate Fracture Dislocations.” eMedicine/Medscape, 22 Sept 2014. Web. Retrieved 16 Sept 2015, from http://emedicine.medscape.com/article/1240108-overview#a10. 3. http://radiologymasterclass.co.uk/tutorials/musculoskeletal/x-ray_trauma_upper_limb/wrist_trauma_x-ray.html (multiple images) 4. http://sfghed.ucsf.edu/Education/ClinicImages/Clin%20L%20finger%20trap%20w%20wts.1.jpg (image) 5. http://www.clicktocurecancer.info/kienbock-disease/ryan-j-grabow-mda-louis-catalano-iii-mdb.html (image) 6. Original case in HPI referred by Dr. Vivek Tayal HPI: Otherwise healthy middle-aged male presents to ED with L arm pain. He fell backwards off a ladder at work bracing the fall with his outstretched L hand. There was immediate pain/swelling to the elbow with inability to range the joint. He denies other injuries, and all vital signs are within normal limits. Exam: L arm adducted w/ elbow held in flexed position. Obvious swelling about elbow joint with prominent olecranon and shortened forearm. Compartments soft, distal motor/sensory function is intact. 2+ radial/ulnar pulses with cap refill <2 seconds. (x-ray shown below) 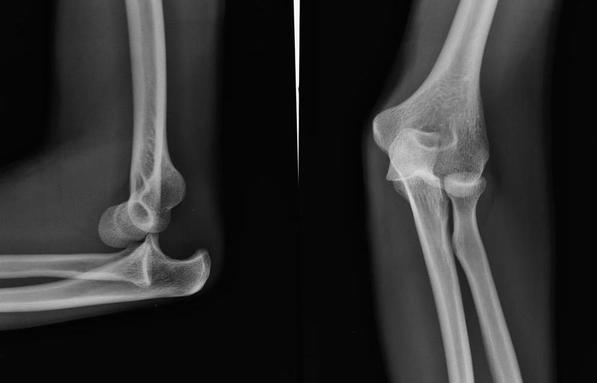 Discussion: Elbow dislocation is the second most common major joint dislocation seen in the ED (behind the shoulder). 80% of elbow dislocations are posterolateral and occur as a combination of: 1) axial loading, 2) forearm supination/external rotation, and 3) posterolateral valgus force to the elbow. · Simple dislocation - no associated fracture (approx 50-60% of cases). · Complex dislocation - one or multiple associated fractures present. Indications for Operative Repair include: 1) complex dislocation, 2) chronic dislocation, or 3) persistently unstable dislocation following attempted reduction. However, acute simple dislocation can typically be treated Non-Operatively w/ closed reduction and splinting. Multiple techniques for reduction exist: Reduction Technique #1 Prone position w/ elbow flexed at 90 degrees and humerus supported by the edge of the stretcher. Apply downward traction to patient’s forearm held in slight pronation, while using your other hand to apply downward and/or medial pressure to the olecranon.  Reduction Technique #2 Supine or seated position w/ elbow held in slight flexion. Perform inline traction while supinating the forearm, with a second provider giving countertraction to the humerus if necessary. Gentle flexion of the elbow and/or medial pressure on the olecranon may be necessary to reduce lateral dislocations.  (YouTube video for demonstration: https://www.youtube.com/watch?v=mlAOGgocRnk)
After successful reduction, perform gentle ROM testing. Inability to range the joint smoothly raises suspicion for fracture, unsuccessful reduction, or re-dislocation. Full elbow extension is not necessary, as the joint is often still unstable in fully extended position. Place a posterior splint w/ forearm in slight pronation and elbow flexed at 90 degrees. Obtain post-reduction films, ensure soft compartments, and confirm intact neurovascular status. Orthopedic follow-up in 7-10 days. Obtain immediate orthopedic consultation for neurovascular compromise, fracture, or reduction failure. Management Pearls: · Plain films to diagnose dislocation and/or need for operative repair · Analgesia/anxiolysis (IV narcotics, hematoma block, +/- procedural sedation) · Successful reduction, gentle ROM, post-reduction films · Confirm intact neurovascular status · Posterior splint, immobilize 7-10 days, f/u with Orthopedics as outpatient By Dr. Blake Johnson References: 1. Aiyer A, Moore D. “Elbow Dislocation” [Web log post]. Retrieved 10 Sept 2015, from http://www.orthobullets.com/trauma/1018/elbow-dislocation. 2. Halstead, M. “Elbow Dislocation.” eMedicine/Medscape, 5 Aug 2014. Web. Retrieved 10 Sept 2015, from http://emedicine.medscape.com/article/96758-overview. 3. Case courtesy of Dr Maulik S Patel, Radiopaedia.org, rID: 14118. http://radiopaedia.org/articles/elbow-dislocation (image 1) 4. Video courtesy of Dr. Fakhouri, MidAmerica Orthopaedics and MidAmerica Hand To Shoulder Clinic. “Posterior Elbow Dislocation & Reduction.” https://www.youtube.com/watch?v=mlAOGgocRnk. 5. http://emedicine.medscape.com/article/96758-workup#c7 (image 2) 6. http://lifeinthefastlane.com/elbow-dislocation/ (image 3) HPI: Middle-aged male with no medical history presents to the ED with a laceration to his left middle fingertip. He was using a circular saw to cut wood this afternoon when he inadvertently cut his left middle finger. He denies other injuries, and all vital signs are within normal limits. Exam: Deep laceration to dorsal surface of distal phalanx on L middle finger involving the lateral nail bed. Full motor/sensory function is intact. Cap refill <2 seconds. Plain films negative for acute fracture/dislocation. (representative image seen below)  Discussion: Fingertip injuries are the most common hand injuries seen in the ED, and evidence shows effective early treatment clearly results in best cosmetic and functional outcomes. Special consideration is taken when injury involves the nail bed. · Germinal Matrix - soft tissue at base of the nail responsible for nail generation/growth. · Sterile Matrix - soft tissue adherent to underside of the nail plate responsible for nail strength/thickness. If nail plate is avulsed or subungual hematoma involves >50% of nail bed, then nail should be removed for hematoma evacuation/irrigation. If underlying laceration involves the germinal or sterile matrix, it should be repaired w/ 6-0 absorbable suture or Dermabond. Soak nail plate in a povidone iodine solution while performing repair. Replace the extracted nail plate at completion to splint the eponychial folds and better mold the edges of the repair for optimal healing (can be sutured in place). Apply a nonadherent dressing and consider a splint to immobilize DIP joint and protect the fingertip. 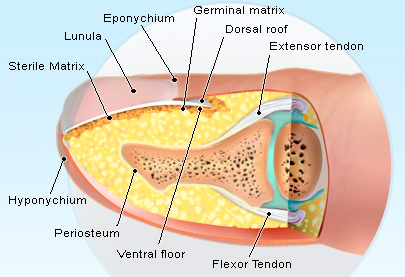 Management Pearls:
· Pain control (digital block), update tetanus status, Abx prophylaxis · Plain films to rule-out distal phalanx fracture · Copious irrigation and close inspection of wound · Nail plate removal and/or nail bed repair as indicated · Replace nail plate to splint eponychial fold and promote nail growth at germinal matrix · Non-urgent orthopedic follow-up as outpatient By Dr. Blake Johnson References: 1. Jones, T. Nail Bed Injury [Web log post]. Retrieved 3 Sept 2015, from http://www.orthobullets.com/hand/6109/nail-bed-injury. 2. Strauss EJ, Weil WM, Jordan C, et al. A prospective, randomized, controlled trial of 2-octylcyanoacrylate versus suture repair for nail bed injuries. J Hand Surg [Am]. 2008 Feb. 33(2):250-3. 3. Yallapragada, R. “Nail Bed Laceration Repair.” eMedicine/Medscape, 25 June 2015. Web. Retrieved 3 Sept 2015, from http://emedicine.medscape.com/article/80792-overview. 4. http://www.sawaccidents.com/table-saw-injury-pictures.htm (image 1) 5. http://www.medicinenet.com/image-collection/fingernail_anatomy_picture/picture.htm (image 2) |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed

{kind=link}