|
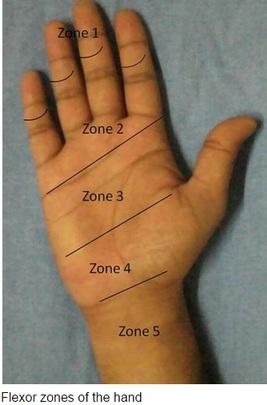
HPI: Approximately 30 y/o right handed male presents with a laceration to base of the left thumb and inability to move his thumb. EXAM: Left hand: Laceration extends along the volar base of the thumb, no other injuries noted. Thumb is held in extension with limited opposition of the thumb. Complete inability to flex the thumb at the ITP. Ability to extend the thumb is preserved. When the wrist is extended, the thumb remains in extension. Decreased two point discrimination distal to the laceration. Ability to cross 2nd and 3rd digits is preserved. Remainder of sensation and motor function of the digits is intact. IMAGES: X-rays are needed only if underlying fracture is suspected (malalignment of digits)
 MANAGEMENT
#ED Management - Assessment for other injuries - Thorough irrigation of wound and closure of skin - Splint in slight flexion - One dose of Ancef preferred - Very close follow up with hand specialist (1-3 days) #Non-Operative - <60% of tendon width affected - Wound care and hand rehab #Operative - >60% of tendon width affected - Ideally within 2 weeks of injury - Extensive hand rehab starting immediately after repair - Lots of repair techniques available depending on zone of injury. Outside the scope of this post DISCUSSION - This patient had a complete FPL transection. Laceration repaired, given 2 day f/u. - Flexor tendons need to be fixed ASAP but not emergently - More urgency than extensor tendon repairs - High suspicion with any volar laceration - Outcomes very variable depending on zone of injury and time until surgery - Hand rehabilitation is paramount to prevent scarring and loss of function - FDP inserts in the DIP. FDS inserts in the PIP. - High probability of concomitant neurovascular injury, associated with worse outcomes - Tenodesis effect - naturally, the digits flex when the wrist is extended. If abnormal very high likelihood of flexor tendon injury. KEY POINTS - High suspicion with volar lacerations and digits in extension - Remember the tenodesis effect - Always check for neurovascular injury - Higher urgency than extensor tendon injuries - Urgent but not emergent surgery required - Can close in the ED and arrange very close hand follow up - Splint in flexion - Be aware of the different different zones of the hand but extensive detail not needed. by Dr. Mohamed El-Kara REFERENCES: http://www.orthobullets.com/hand/6031/flexor-tendon-injuries
0 Comments
HPI: 55 y/o male with history of etoh abuse and bilateral THA presents with left hip pain and inability to walk. He has been drinking etoh and playing with his grandchildren when he noticed his left hip dislocated. This occurs monthly. EXAM: Left leg is slightly shorter than right. Leg and hip in flexion, adduction, and internal rotation. Able to palpate the femoral head. No deficits of foot function noted. IMAGES: Obtain AP and Lateral Hip  MANAGEMENT:
#Non-operative - First line when no associated fractures are present - Frequently requires sedation but not paralyzation (unlike traumatic which requires both) - Flex the hip and knee to 90 degrees, place axial traction, internally rotate the hip with a second person placing counter traction on the hip - Second person can help guide the femoral head into proper positioning - Place in knee immobilizer post reduction to prevent recurrence #Operative - Indications include inability to reduce non-operatively, associated fractures, multiple dislocations - Revision of THA can occur as an outpatient and does not require admission DISCUSSION: - Posterior dislocation occurs in 75-90% of cases - Risk factors: prior hips surgery, etoh abuse, age >70, malpositioning of components, etoh abuse, neuromuscular disease - Mechanism: hip flexion, adduction with internal rotation. (ie: shoe tying, sitting on toilet) - Easier to reduce than traumatic dislocations, should not require paralytics - Fracture of the femur is a complication of the procedure, especially with predisposing diseases (etoh abuse, chronic steroids) - AT CMC, protocol is to reduce in PACU under sedation - Can d/c home following reduction with ortho follow up - Anterior dislocations can be reduced with axial traction and internal rotation without flexion of the hip. KEY POINTS: - 90% posterior dislocations (hip in flexion, adduction, internal rotation) - Hip x-rays to assess for dislocation type and for fractures - Frequently only requires sedation without paralytics - Reduction by hip/knee flexion to 90 degrees, axial traction and internal rotation - Frequently requires a lot of force to reduce - Place in knee immobilizer post reduction to prevent recurrence - Don’t break the femur by Dr. Mohamed El-Kara References: http://medapparatus.com/Ortho/Images/JointArthroplasty/DislocatedLeftHipArthroplasty.jpg http://www.orthobullets.com/recon/5012/tha-dislocation HPI: 5 year old female presents with right arm pain after falling on a chair. Her arm was pinned in between the chair and the floor. She had immediate pain but it resolved. The following day she has increased pain and swelling in the right arm. EXAM: Swelling is noted in the proximal forearm. Tenderness to palpation present on the proximal ulna as well as radial head. No tenderness to the medial condyle, lateral condyle, or olecranon. Passive and active range of motion of the elbow is full but painful. No motor or sensory deficits of the hand. IMAGING. AP and lateral views of the elbow.   Note there is plastic deformation of the ulna without a complete fracture
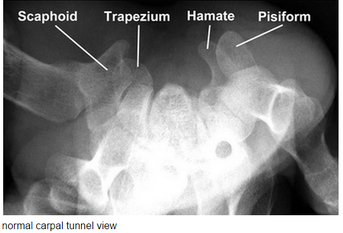
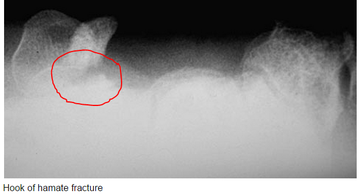
Always assess the radial head, it should point towards the capitulum MANAGEMENT #Non-operative - Closed reduction of ulna and radial head dislocation and long arm casting - If no ortho available, attempt to reduce radial head and place in a posterior splint. - Axial traction traction to restore ulnar length - Need to successfully reduce radial head dislocation as well - Immobilize in 110 degrees flexion and full supination. #Operative - Indicated if radial head or ulnar length are unstable following reduction - Indicated in Bado Type IV fractures (complete fx of Ulna and Radius) - Frequently required in missed diagnosis. DISCUSSION - A Monteggia fracture is radial head dislocation plus a proximal ulna fracture or plastic deformation of the ulna - Peak age range 4-10 years, fall onto pronated arm.. - Frequently missed since the ulna may only have plastic deformation, have a high suspicion if there is pain over the radial head or evidence of radial head dislocation. - Complications include posterior interosseous nerve neurapraxia (finger drop, radial wrist deviation). - Loss of forearm motion with delayed treatment (2-3 weeks) - Different classifications are present (Bado) but not as key as recognizing the fracture. - This patient was casted and follow up arranged. KEY POINTS - Have a high index of suspicion when there is radial head tenderness or dislocation - Ulna may show only plastic deformation - Radial head should always point towards the capitulum - Obtain contralateral arm films if comparison is needed. - ED management without ortho includes reduction with posterior splint placement. Close f/u. - Majority of cases result in non-operative management. - Frequently missed By Dr. Mohamed El-Kara REFERENCES http://www.orthobullets.com/pediatrics/4015/monteggia-fracture--pediatric http://emedicine.medscape.com/article/415822-overview#a5 HPI: Young adult presents with distal left 5th digit discoloration after a sporting event. He felt intermittent sharp pain in the ulnar portion of his left hand but otherwise no other complaints immediately following the injury. The following day, he had discoloration of his left 5th digit but the pain resolved. EXAM: Purplish discoloration present in the left 5th digit distal to the DIP. Allen’s test reveals reduced ulnar blood flow. No pain to palpation of any portion of the hand. Flexion/extension intact in all left hand joints. 2 point discrimination reduced in the left 5th digit. Doppler flow present in the superficial blood vessels. IMAGING: Best seen with a carpal tunnel view. Also obtain an AP view.
MANAGEMENT:
Non-operative - Acute hook or body fractures - 6 weeks immobilization Operative - Excision of hamate fracture fragment - Chronic hook of hamate with non-union - neurovascular compromise - ORIF with very little benefit DISCUSSION/PEARLS: - This was most likely a chronic fracture with resulting non-union and was reinjured. - Surgical findings included engorged veins and arteries - Associated with golf and baseball injuries - Usual presentation: Hypothenar pain to palpation - Pain with tight grip and decreased grip strength - In Chronic cases: Ulnar nerve compression resulting in 4th, 5th digit paresthesias - Rarely: Ulnar artery thrombosis KEY POINTS - Consider with ulnar sided hand pain with golf and baseball injuries - Pain with grip strength - Obtain a carpal tunnel view - Hamate body fracture very rare, hook fracture much more common - Non-union results in chronic ulnar nerve symptoms - Non-operative management is appropriate if acute without any neurovascular compromise - Operative management involves excision of fractured portion. By Dr. Mohammad El Kara REFERENCES: http://openi.nlm.nih.gov/detailedresult.php?img=2904904_256_2009_842_Fig1_HTML&query=null&req=4&npos=-1 http://www.orthobullets.com/hand/6035/hook-of-hamate-fracture |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed

{kind=link}