|
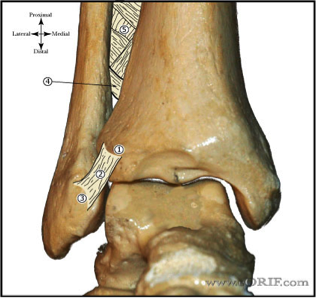
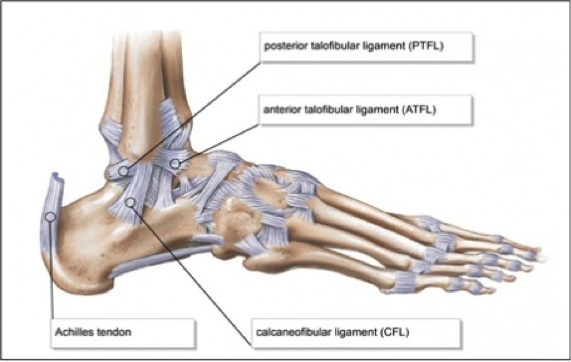
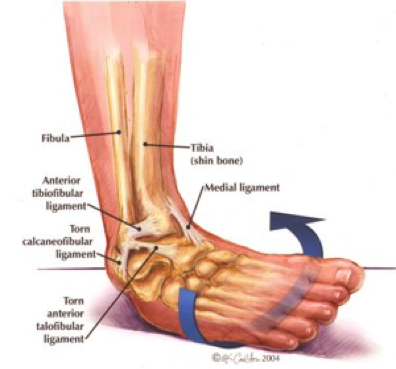
In order to begin an appropriate assessment of the ankle, it is necessary to review the significant anatomical structures. Bony Anatomy First, we have the two long bones that form the proximal portion of the joint – the tibia and the fibula. At the ankle joint, the tibia extends as the lateral malleolus and posterior malleolus while the fibula forms the medial malleolus. The distal boney structure of the joint is formed by the talus. 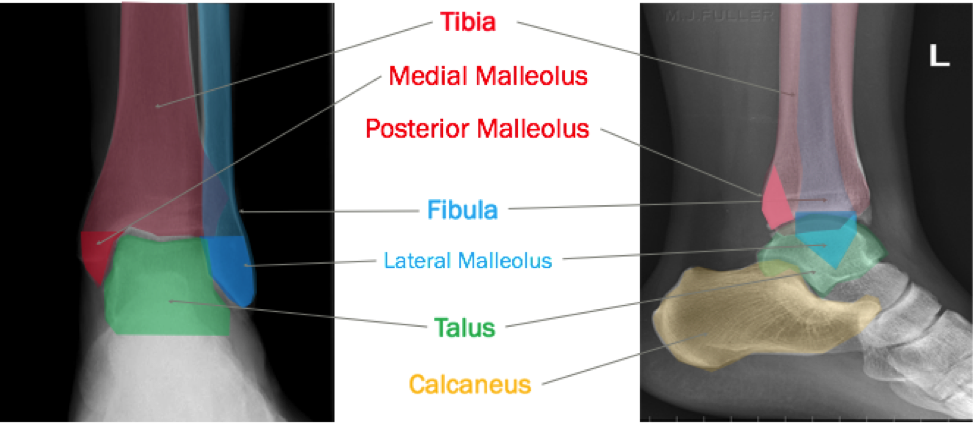 Joint Anatomy A majority of the articular surface is formed by the horizontal portion of the distal tibia (the tibial plafond) which extends parallel to the dome of the talus; taken with the medial and lateral malleoli, it forms a rectangular socket known as the ankle mortise. Being a synovial joint, the ankle joint (between the ankle mortise and talar dome) is surrounded by a joint capsule. Like the knee joint capsule, the ankle capsule has an additional cranial extension at the syndesmosis. 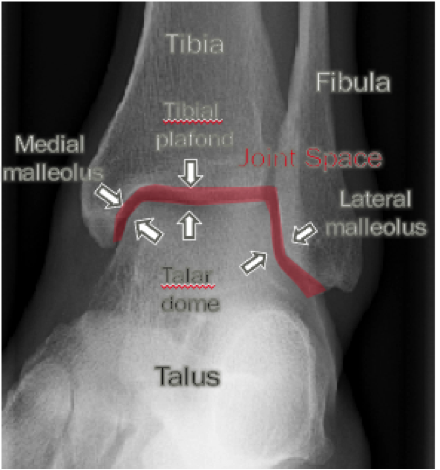 Ligament Anatomy The lateral and medial malleoli have ligamentous attachments to the talus and calcaneus that contribute to stability of the joint.

 Initial Evaluation A patient presenting with a suspected ankle injury should undergo the following assessment:
Our initial evaluation is important because it helps utilize the following decision tool: Ottawa Ankle Rule The Ottawa Ankle Rule helps us screen for patients that will benefit from ankle imaging. Ankle Imaging is warranted in those who have ankle pain and:
Tips from the creators at University of Ottawa: Palpate the entire distal 6cm of the fibula and tibia; Do not neglect the importance of medial malleolar tenderness; “Bearing weight” counts even if the patient limps; Be caution in patients under age 18. Imaging Studies When imaging the ankle obtain 3 views to appropriately evaluate the joint: AP, Lateral and the Mortise study.  Radiographic Evaluation Begin with the AP and Lateral views. Trace the entire length of the tibia and fibula paying special attention to the fibula on the lateral view, for oblique fractures may be difficult to see. Next, proceed to the mortise view. Trace around the mortise and Talar dome, evaluate for joint space uniformity. The ring structure of the ankle is made up of three bones (tibia, fibula and talus) and three ligaments (medial and lateral collateral ligaments and interosseous ligament) if there is one break in the ring, look for a second. To evaluate the integrity of the syndesmosis use the following measurements: •Tibiofibular overlap < 1mm •Increased medial clear space: less than or equal to 4 mm •Increased Tibiofibular clear space: < 6 mm  Additional radiographic measurements Talo-crural angle : The angle is formed by drawing a line parallel to the tibial plafond, a line perpendicular to the tibail plafond, and a line connecting the lateral and medial malleoli. This angle should be between 75 – 87 degrees and should be within 2-5 degrees of contralateral side. Deviation from these measurements is indicative of fibula shortening.  Typical Fracture Patterns Isolated Medial Malleolus Fracture 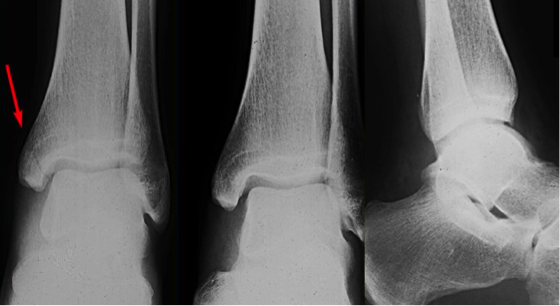 Isolated Lateral Malleolus Fracture  Isolated Posterior Malleolus Fracture  Bimalleolar fracture / equivalent  *Notice how there are two breaks to the ring structure, therefore this injury pattern is consistent with an unstable joint (increased medial clear space, distal fibula fracture). These unstable injuries convey a higher need for orthopedic intervention. Associated syndesmotic injuries
Pilon Fracture This following fracture pattern is often confused for an ankle fracture, however the presence of a pilon fracture conveys a different mechanism and prognosis. A Pilon fracture, French for mortar and pestle, occurs due to an axial loading mechanism and is defined by articular impaction and comminution of the distal tibia. When you see a pilon fracture it is important to evaluate for other injuries typical of axial loading (i.e. lumbar spine, calcaneus, ect.) 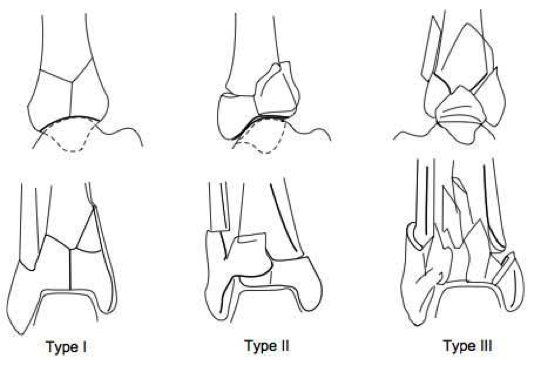
Sources https://radiopaedia.org/articles/ankle-radiograph-an-approach http://www.orthobullets.com/trauma/1047/ankle-fractures http://www.orthobullets.com/trauma/1046/tibial-plafond-fractures?expandLeftMenu=true https://radiopaedia.org/search?utf8=✓&q=pilon+fracture&scope=all https://meds.queensu.ca/central/assets/modules/ts-ankle-radiograph/isolated_medial_malleolus_fracture.html BY: DR. ETHEN ELLINGTON M.D.
2 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|




 RSS Feed
RSS Feed
