|
HPI: Patient 1: Restrained passenger of a head on MVC. Patient 2: Elderly patient with fall from standing. Physical Exam: Patient 1: Hip flexed and internally rotated. Unable to straighten the leg. Unable to walk. Patient 2: Hip flexed and externally rotated. Unable to straighten the leg. Unable to walk. Imaging: Patient 1: Posterior hip dislocation of native hip. Patient 2: Superolateral hip dislocation of prosthetic hip. Posterior Hip Dislocation
Prosthetic Hip Dislocation
Treatment:
****Don't forgot you can find the ED Policy for Deep Sedation on the Top 20 Page. Anesthesia must be present for intubation. Click here to read more.
0 Comments
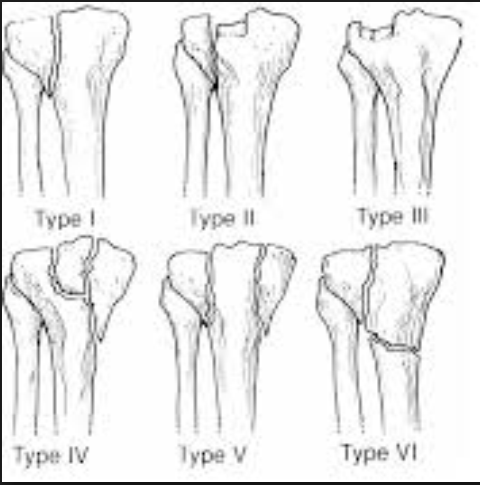
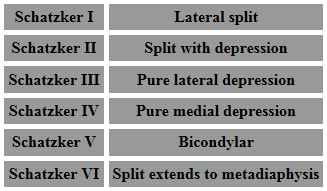
HPI: Patient 1: Restrained MVC. Presented with knee pain and swelling. Patient 2: Fall from height and chief complaint of shoulder and knee pain. Physical Exam: Patient 1: Swollen left knee with tenderness to palpation. Patient 2: Knee visibly deformed, swollen, and bruised. Small open deformity w/ active bleeding. High risk for compartment syndrome. Imaging: Patient 1: Schatzker type 2 fracture (see table below for classifications of Schatzker fracture) Patient 2: Schatzker type 6 fracture
Dispo: Patient 1: Admitted. Splinted w/ ORIF as inpatient. Patient 2: Admitted. Splinted w/ closed reduction and external fixation. Plan for definitive repair in ~2 weeks after soft tissue swelling has subsided. Treatment: 1) Hinged knee brace w/ passive ROM - for patients w/ minimally displaced or split depressed fractures or minimal baseline mobility. 2) External fixation - for patient w/ open or comminuted fractures or significant soft tissue swelling. 3) ORIF - for >3mm articular step off or varus/valgus instability. Types of Schatzker Fractures:
HPI: Patient presents with a grossly deformed right upper extremity. PE: Gross deformity of humerus, no open fracture. Unable to extend wrist. Unable to hyper-extend MP joints of fingers and unable to flex IP joint of thumb. Radial and ulnar pulses intact. IMAGING: Multi-factorial fracture along the mid third of humerus along the expected course of the radial nerve. DISPO (if at free standing ED): Transfer patient to ED with on-call orthopedics for definitive fixation. Reduce and splint prior to transfer. TREATMENT: Nonoperative managment. Splinted and cast at bedside. Follow radial nerve palsy clinically for improvement.  |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|


 RSS Feed
RSS Feed
