|
HPI: Middle age male who presents after falling at work. His medial forearm stroke a metal bucket just distal to his elbow and resulted in a large laceration. PE: Patient is unable to flex at the DIP of digit 4 and 5. He is unable to cross the second and third fingers or adduct his fingers. He has decreased sensation over the medial aspect of the 4th and 5th digit. Suspected ulnar nerve laceration.  Anatomy: Derives from the medial portion of the brachial plexus (C8-T1). It lies posteromedial to the brachial artery in the upper arm and traverses behind the medial epicondyle. The ulnar nerve runs along on the ulnar aspect of the wrist along with the ulnar artery. It passes through Guyon’s canal where it bifurcates into sensory and deep motor branches. 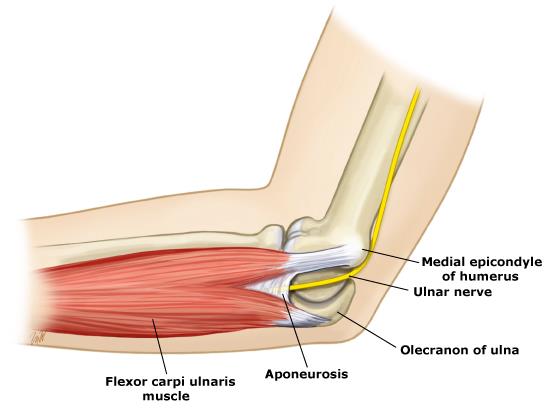 Innervation:
- Motor:
- Sensory:
Clinical conditions:
Treatment: Forearm exploration with transected nerve repair. Pearls:
0 Comments
HPI: 7 y/o fall from monkey bars. Landed on extended shoulder + outstretched arm. Physical exam: Obvious arm deformity. Ecchymosis over distal/medial arm. Inability to flex thumb IP joint and DIP of index finger (AIN neuropraxia). Palpable pulses. Warm extremity. 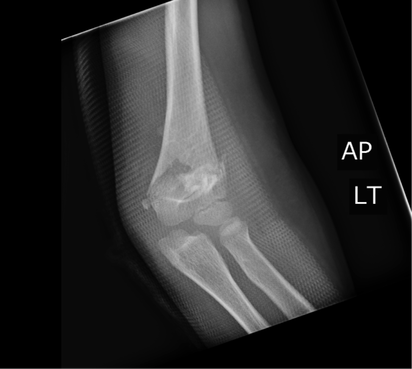
AP showing mild varus angulation 
Lateral film showing significant posterior displacement of distal portion of fracture 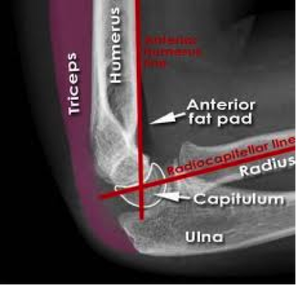
Normal lateral film 
Normal AP flim showing Baumann's angle: angle btw humerus and capitellar physis. This measures amount of varus/valgus deformity Supracondylar Humerus Fractures:
Two categories: · Extension: Distal fragment displaced anteriorly (95% of cases). · Flexion: Distal fragment displaced posteriorly (5% of cases). Four Types: · I: Nondisplaced: look for posterior fat pad · II: Displaced. Posterior cortex intact · III: Completely displaced · IV: Complete periosteal disruption with instability on flexion and extension. Presentation: · Usually from fall on outstretched hand. · Frequently will have neurologic findings: · Anterior Interosseus Neuropraxia: · Most common neurologic finding. Particularly with extension-type fractures. · AIN is a branch of Median nerve. · Patient's cannot flex thumb IP joint or index DIP joint (Can't make an “OK” sign). Almost all will resolve with conservative management. Also have vascular compromise in approximately 1% Usually brachial artery compromise High collateral flow, so patient may have a pink, but pulseless extremity. Still requires emergent reduction. Treatment: Type I: Immobilization at 90 degrees and ortho follow-up. Type II: Closed reduction unless displacement is minimal. Adequate reduction: Baumann's angle wnl, anterior humeral line transects capitellum Type III: High-risk for neurovascular complications. Get ortho involved. Almost always require closed reduction + pinning vs. open reduction Type IV: Open surgical reduction and fixation Indications for open reduction: 1.) Inadequate reduction with closed techniques 2.) Vascular injury 3.) open fracture 4.) Type iv fracture HPI: Patient presents with a grossly deformed right upper extremity. PE: Gross deformity of humerus, no open fracture. Unable to extend wrist. Unable to hyper-extend MP joints of fingers and unable to flex IP joint of thumb. Radial and ulnar pulses intact. IMAGING: Multi-factorial fracture along the mid third of humerus along the expected course of the radial nerve. DISPO (if at free standing ED): Transfer patient to ED with on-call orthopedics for definitive fixation. Reduce and splint prior to transfer. TREATMENT: Nonoperative managment. Splinted and cast at bedside. Follow radial nerve palsy clinically for improvement.  |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
