|
HPI: Middle age man s/p MCC with open fracture of right leg. Tourniquet applied in the field. Physical Exam: Completely shattered tibia and fibula with 10cm open wound. Weak but palpable DP after taking tourniquet down. Intact sensation to light touch in superficial peroneal, deep peroneal, and tibial distributions. Able to wiggle toes and slight dorsiflexion. Management: Basic Management of Open Fractures
0 Comments
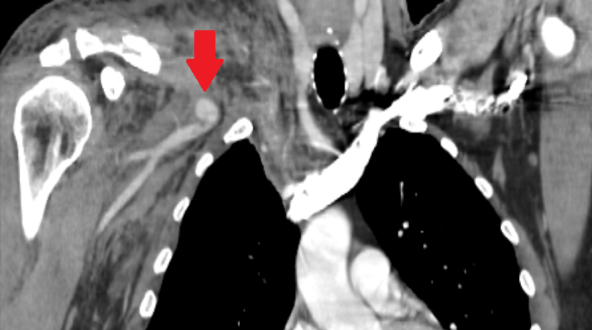
HPI: Middle age male who presented as an adult trauma code after a fall off a horse. Patient with significant pain in right shoulder and anterior upper chest. No numbness or tingling to the right upper extremity. No weakness to the right upper extremity. Physical Exam: significant deformity, edema, ecchymosis, tenderness to right clavicle. Normal strength with the exception of limited shoulder abduction secondary to pain on the right, normal sensation in the right upper extremity. Radial pulse 1+, biphasic on doppler on the right. Radial pulse 2, triphasic on doppler on left. Radiology: X-Ray Clavicle: oblique fracture of distal third of the right clavicle with inferior displacement of distal fragment. Associated R acromion fracture (see figure) CTA Chest: 12 mm right subclavian artery pseudoaneurysm, suspect right subclavian view transection. Right sided ribe fractures and pneumothorax.
Management: Patient had a chest tube place, and was admitted to the STICU. Orthopedic surgery and Vascular surgery were consulted for his right clavicle fracture with underlying pseudoaneurysm. He underwent subclavian artery stenting by vascular surgery. In regards to his clavicle fracture, he was placed in sling for comfort, made non-weight bearing to right upper extremity. No operative intervention was performed. Discussion: Clavicle fractures are very common and account for 5-10% of all fractures. Vast majority of clavicle fractures are managed non-operatively and, with VERY few exceptions, nearly all clavicle fracture can be discharged to home from the ED with outpatient follow up if they, in the rare occasion, do require surgery. 80% of clavicle fractures involve the middle third of the clavicle. Without any associated neurovascular injury, these all can be discharged to home. Patient is likely to undergo outpatient surgery if there is greater than 100% displacement. The main associated injuries to rule out with clavicle fracture are: 1. subclavian artery/vein injury (suspect in patients with abnormal UE vascular exams, as presented in this patient case!) 2. floating shoulder, or scapulothoracic dissociation (suspect in patients with significantly widened or distracted fractures) 3. skin tenting (most patients, will have palpable deformity of clavicle with edema than may be confused for skin tenting—true skin tenting is when the skin is stretched to the point that is causes vascular compromise and skin discoloration) 4. pneumothorax (suspect in patients with significantly displaced clavicle fractures) 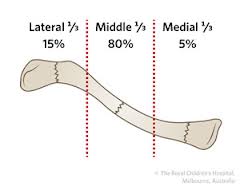
HPI: Middle age male who presents with left index finger pain and swelling after injury involving high pressure paint spray gun. He has had increasing pain and swelling to distal portion of the finger since the incident 72 hours prior. Physical Exam: Edema, warmth, erythema and purple discoloration to middle and distal phalanx of left index finger. Tenderness to palpation. Unable to flex and extend at DIP secondary to pain. (See image). Afebrile. No other significant findings. Imaging: no fracture or dislocation. Increased attenuation in soft tissues below second distal phalanx (see image)
Management: This patient had no fracture or dislocation and a relatively benign appearing exam. However, given mechanism of injury and high risk of underlying injury with high pressure injection injuries, patient was admitted to Ortho Hand Service. He was given clindamycin and tetanus vaccination. He was taken to the operating room for incision and washout. Significant damage to underlying fascia and tissue found with presence of white latex-type paint. Patient did well post-op with out complications.
Key Points:
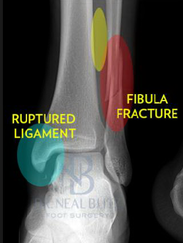
HPI: Middle age male who presents with left ankle pain, swelling, and deformity s/p fall down stairs. Unable to bear weight to LLE. Physical Exam: obvious deformity, edema, ecchymosis to L ankle. TTP over medial and lateral malleolus. Unable to flex and extend at ankle 2/2 pain. DP/PT 2+. Normal sensation to light touch to dorsal surface/plantar surface/1st web space. IMAGING:
Diagnosis and Management: This patient has a Weber B distal fibula fracture with medial subluxation of the tibia and disruption of the mortise joint. Combination of distal fibula fracture and likely complete disruption of deltoid ligament is a bimalleolar fracture-dislocation equivalent. Thus, this is an UNSTABLE ANKLE! Patient’s ankle was reduced using axial traction and inversion, placed in posterior sugar tong splint. Injury required 3 reductions, which is common due to the instability of this injury. Patient was admitted to Orthopedic Trauma service and scheduled for next day ORIF.
|
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|







 RSS Feed
RSS Feed
