|
HPI: Otherwise healthy middle-aged male presents to ED with L hand pain. He is a painter, and while cleaning a high-pressure pneumatic pain gun it accidentally discharged into the palm of his L hand. He reports only moderate pain at the site. Denies any other injuries, all vital signs within normal limits. Event occurred 2 hours prior to ED arrival. Exam: Pin-hole size puncture wound on palmar surface of hand w/ moderate tenderness to palpation and minimal surrounding erythema. Full passive/active ROM of all digits, neuromuscular function completely intact. Cap refill <2 seconds in all 5 digits. X-ray is unremarkable.  Discussion: High-Pressure Injection Injuries occur when a high-pressure injection device (pneumatic paint gun, grease gun, diesel injector, etc) injects into the operator. Most common in male laborers in painting and automotive industries, and injury often occurs during cleaning of the device or while attempting to clear the nozzle. Non-dominant hand involved ~75% of the time, with index finger injury most common, followed by middle finger and palm. Despite benign outward appearance, there is almost always significant underlying damage, and should be considered a SURGICAL EMERGENCY. Our job as ED providers is to recognize the seriousness of the injury and involve a hand surgeon as fast as possible! Pathophysiology involves direct trauma resulting in local tissue damage, acute and chronic inflammation, and foreign body granuloma formation. Tissue ischemia/necrosis from vascular compression, chemical inflammation, and secondary infection can lead to devastating functional outcomes, including amputation. Key historical details that impact prognosis:
Time from injury to treatment is the most important prognostic factor. Delay of >10 hours significantly increases risk of amputation. Higher PSI and larger volume of injected material portend greater direct tissue damage. Hydrocarbon-based substances (fuel, organic solvents, oil-based paint, paint thinners) cause more severe inflammatory reaction and tissue necrosis, with amputation rates >50%. Grease, latex, and water-based paints re typically less destructive. Obtain plain films in the ED to rule out coexistent fracture/dislocation. Some injected materials may appear radiopaque on x-ray and could aide in pre-operative planning. Administer broad-spectrum parenteral antibiotics in the ED, and update tetanus status. Control pain as needed, and arrange for emergent orthopedic/hand surgery evaluation. Transfer to Trauma Center if necessary. Patient will need emergent operative irrigation and debridement. Patient in HPI above had excellent functional outcome due to early presentation. Below is a time-course representation of patient with a delayed presentation, outlining potential damage that can occur. 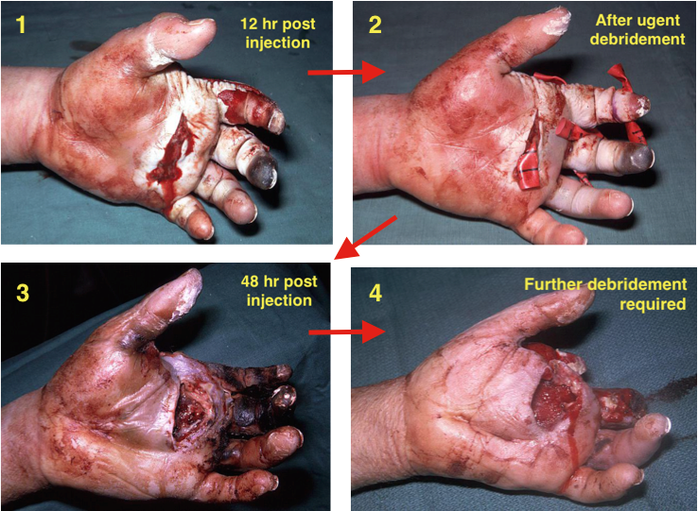 Management Pearls:
By Dr. Blake Johnson References: 1. Aiyer, A. "High-Pressure Injection Injuries." OrthoBullets, 15 Mar 2014. Web. Retrieved 25 Sept 2015, from http://www.orthobullets.com/hand/12104/high-pressure-injection-injuries. 2. Sanford, S. "High-Pressure Hand Injury." eMedicine/Medscape, 12 Nov 2013. Web. Retrieved 25 Sept 2015, from http://emedicine.medscape.com/article/826620-overview. (multiple images) 3. http://lifeinthefastlane.com/high-pressure-injection-injury/ (image)
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
