|
HPI: Otherwise healthy middle-aged male presents to ED with L arm pain. He fell backwards off a ladder at work bracing the fall with his outstretched L hand. There was immediate pain/swelling to the elbow with inability to range the joint. He denies other injuries, and all vital signs are within normal limits. Exam: L arm adducted w/ elbow held in flexed position. Obvious swelling about elbow joint with prominent olecranon and shortened forearm. Compartments soft, distal motor/sensory function is intact. 2+ radial/ulnar pulses with cap refill <2 seconds. (x-ray shown below) 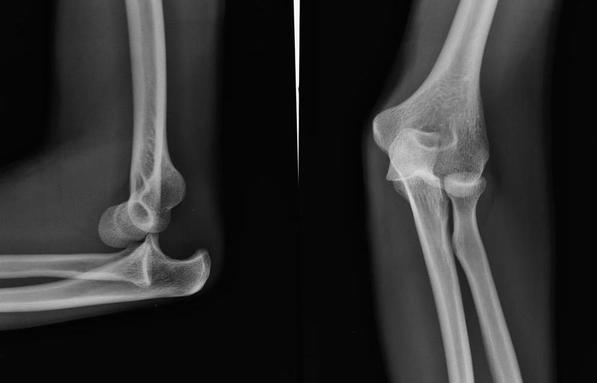 Discussion: Elbow dislocation is the second most common major joint dislocation seen in the ED (behind the shoulder). 80% of elbow dislocations are posterolateral and occur as a combination of: 1) axial loading, 2) forearm supination/external rotation, and 3) posterolateral valgus force to the elbow. · Simple dislocation - no associated fracture (approx 50-60% of cases). · Complex dislocation - one or multiple associated fractures present. Indications for Operative Repair include: 1) complex dislocation, 2) chronic dislocation, or 3) persistently unstable dislocation following attempted reduction. However, acute simple dislocation can typically be treated Non-Operatively w/ closed reduction and splinting. Multiple techniques for reduction exist: Reduction Technique #1 Prone position w/ elbow flexed at 90 degrees and humerus supported by the edge of the stretcher. Apply downward traction to patient’s forearm held in slight pronation, while using your other hand to apply downward and/or medial pressure to the olecranon.  Reduction Technique #2 Supine or seated position w/ elbow held in slight flexion. Perform inline traction while supinating the forearm, with a second provider giving countertraction to the humerus if necessary. Gentle flexion of the elbow and/or medial pressure on the olecranon may be necessary to reduce lateral dislocations.  (YouTube video for demonstration: https://www.youtube.com/watch?v=mlAOGgocRnk)
After successful reduction, perform gentle ROM testing. Inability to range the joint smoothly raises suspicion for fracture, unsuccessful reduction, or re-dislocation. Full elbow extension is not necessary, as the joint is often still unstable in fully extended position. Place a posterior splint w/ forearm in slight pronation and elbow flexed at 90 degrees. Obtain post-reduction films, ensure soft compartments, and confirm intact neurovascular status. Orthopedic follow-up in 7-10 days. Obtain immediate orthopedic consultation for neurovascular compromise, fracture, or reduction failure. Management Pearls: · Plain films to diagnose dislocation and/or need for operative repair · Analgesia/anxiolysis (IV narcotics, hematoma block, +/- procedural sedation) · Successful reduction, gentle ROM, post-reduction films · Confirm intact neurovascular status · Posterior splint, immobilize 7-10 days, f/u with Orthopedics as outpatient By Dr. Blake Johnson References: 1. Aiyer A, Moore D. “Elbow Dislocation” [Web log post]. Retrieved 10 Sept 2015, from http://www.orthobullets.com/trauma/1018/elbow-dislocation. 2. Halstead, M. “Elbow Dislocation.” eMedicine/Medscape, 5 Aug 2014. Web. Retrieved 10 Sept 2015, from http://emedicine.medscape.com/article/96758-overview. 3. Case courtesy of Dr Maulik S Patel, Radiopaedia.org, rID: 14118. http://radiopaedia.org/articles/elbow-dislocation (image 1) 4. Video courtesy of Dr. Fakhouri, MidAmerica Orthopaedics and MidAmerica Hand To Shoulder Clinic. “Posterior Elbow Dislocation & Reduction.” https://www.youtube.com/watch?v=mlAOGgocRnk. 5. http://emedicine.medscape.com/article/96758-workup#c7 (image 2) 6. http://lifeinthefastlane.com/elbow-dislocation/ (image 3)
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
