|
HPI: Otherwise healthy middle-aged male presents to ED with L wrist pain following moderate speed motorcycle collision. There was immediate pain/swelling to L wrist, and he is reluctant to range the joint. He was helmeted and wearing full protective clothing. Denies other injuries, all vital signs within normal limits. Exam: Prominent L wrist swelling. Dorsal aspect of radial head firmly palpated beneath the skin with slight volar displacement of hand relative to forearm. Skin intact, compartments are soft. Radial and ulnar pulses palpable, distal cap refill <2 seconds. Distal motor function intact, slightly diminished sensation in median nerve distribution of L hand. (X-ray shown below) 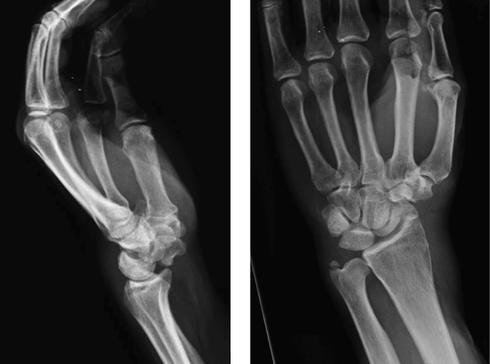 Radiologist Interpretation: Perilunate dislocation. Concomitant scaphoid waist fracture (central third) w/ distal anterior displacement. Minimally displaced ulnar styloid fracture. Discussion: Lunate dislocation (perilunate dissociation) is a high-energy injury with poor functional outcomes that almost universally requires operative intervention. Unfortunately they are commonly missed on initial presentation (~25%) due to subtleties on radiographic imaging. First, a review of normal carpal anatomy, characterized by 3 smooth lines called Gilula’s arcs: 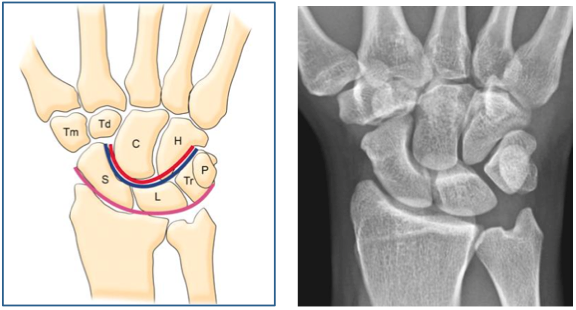 Any disruption in Gilula’s arcs raises suspicion for carpal fracture/dislocation. Lateral wrist film is essential to confirm normal in-line alignment of the radius, lunate, and capitate: 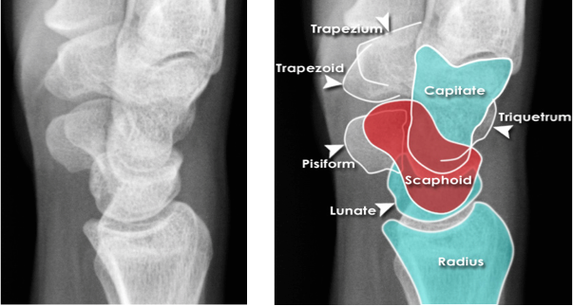 Mechanism of lunate dislocation typically involves high-energy axial load to the wrist, trapping the hand in hyperextension with ulnar deviation. Results in relative intercarpal supination causing varying degrees of carpal ligamentous rupture and articular dissociation. Injury pattern occurs in a step-wise sequence of events corresponding to Mayfield Classification System: · Stage I -> Scapho-lunate dissociation (SL widening) · Stage II -> Above w/ luno-capitate disruption (capitate overrides lunate) · Stage III -> Above w/ luno-triquetral disruption (true “perilunate dissociation”) · Stage IV -> Lunate completely dislocated from lunate fossa (usually volar, i.e. “spilled tea cup sign”) 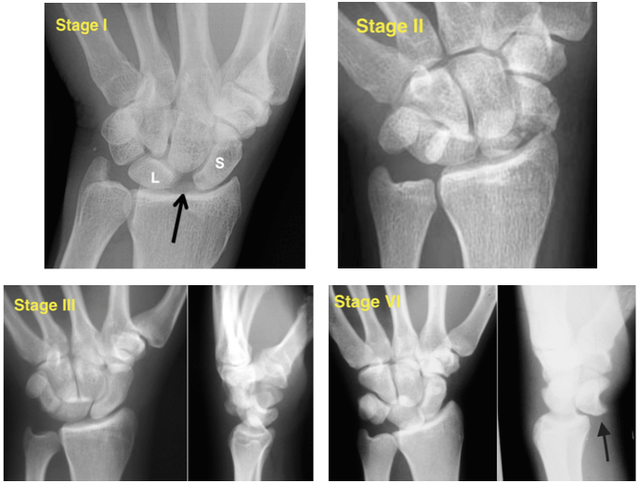 In addition to pain, stage IV dislocation and/or surrounding wrist fracture-dislocation can present with carpal tunnel compression and median nerve symptoms (~25% of patients). Emergent orthopedic consultation recommended. Closed reduction is performed in the ED using fingertraps to apply traction and to distract carpal bones while applying a sugar tong splint (may be all that is necessary). For complete lunate dislocations (stage IV), lunate must be relocated back into lunate fossa: 1) Apply gentle traction w/ wrist slightly extended 2) Manual pressure to palmar projection of lunate while flexing wrist until “snap” occurs (indicates relocation as proximal pole of capitate overcomes dorsal lip of the lunate) 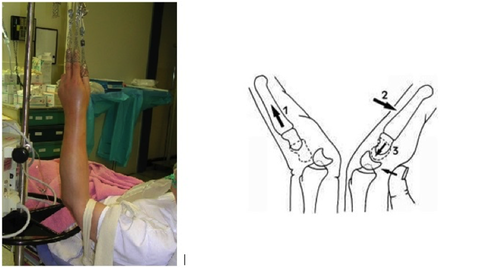 All acute lunate/perilunate dislocations require operative treatment with ORIF, ligament repair, and possible carpal tunnel release. There is universally poor functional outcomes with non-operative treatment, and recurrent dislocation is the rule, not the exception.
Management Pearls: · Know radiographic pathoanatomy, EASY TO MISS! · Assess for median nerve pathology and vascular injury · Emergent orthopedic consultation · Closed reduction with finger traps, apply sugar tong splint · Likely does not require admission, but operative treatment ASAP · High energy mechanism, don’t miss coexistent fracture or other injuries By Dr. Blake Johnson References: 1. Karadsheh, M. “Lunate Dislocation (Perilunate Dissociation).” OrthoBullets, 24 Dec 2014. Web. Retrieved 16 Sept 2015, from http://www.orthobullets.com/hand/6045/lunate-dislocation-perilunate-dissociation. (multiple images) 2. Murray, P. “Perilunate Fracture Dislocations.” eMedicine/Medscape, 22 Sept 2014. Web. Retrieved 16 Sept 2015, from http://emedicine.medscape.com/article/1240108-overview#a10. 3. http://radiologymasterclass.co.uk/tutorials/musculoskeletal/x-ray_trauma_upper_limb/wrist_trauma_x-ray.html (multiple images) 4. http://sfghed.ucsf.edu/Education/ClinicImages/Clin%20L%20finger%20trap%20w%20wts.1.jpg (image) 5. http://www.clicktocurecancer.info/kienbock-disease/ryan-j-grabow-mda-louis-catalano-iii-mdb.html (image) 6. Original case in HPI referred by Dr. Vivek Tayal
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed

{kind=link}