hpiA 15 yr old female right hand dominant with no significant past medical history presents with left shoulder pain after sustaining injury while playing basketball. States she can not clearly recall the events but remembers extending her arm for the ball and having sudden onset of pain. Describes generalized constant aching pain to the left shoulder only. She has been unable to range her left shoulder since the event stating “it hurts too much”. She denies any numbness or tingling. No other complaints. Last PO intake approximately 6 hours ago. physical examGeneral: adolescent female sitting upright in bed with left arm flexed and adducted, moderate distress LUE: left arm held flexed and adducted against her body. Square-like appearance to the shoulder compared to the right which appears rounded. No erythema, abrasions, lacerations, or ecchymosis. Unable to flex, extend, or abduct left shoulder due to pain. Full flexion and extension of elbow and wrist. She can make thumbs up, okay sign, cross fingers, touch thumb to pinky, and keep fingers spread against resistance. Sensation intact in the median, ulnar and radial nerve distributions. Sensation intact in the axillary nerve distribution. 2+ radial pulse radiograph diagnosis and treatmentAnterior left shoulder dislocation. She was given intranasal fentanyl, intraarticular lidocaine and nitrous oxide. Left shoulder was then reduced by external rotation with elbow at patient’s side. No complications. Post reduction films obtained show successful reduction with no fractures discussionAnterior shoulder dislocations are the most common shoulder dislocation, accounting for approximately 95%. Majority of these occur in patients younger than 30 years old. Posterior dislocations account for about 5%, and inferior dislocations (luxation erecta) are extremely rare. Anterior shoulder dislocations occur secondary to a “hyper” external rotation. The glenoid dislocates to the position of either subcoracoid (90%), subclavicular, or sublenoid. Usually the patient holds arms by their side. In a thin patient, the acromion appears prominent giving the classic “squared off” appearance the shoulder. In larger patients, the effected shoulder may appear more round instead of its normal square shape. Intra-articular lidocaine can be used for pain relief prior to reduction as shown below.  Nitrous oxide is also a common and effective means for pain relief. A full neurovascular exam is crucial, approximately 13.5% will have neurologic injury. Axillary nerve is the most commonly effected. This nerve is tested by assessing pinprick sensation over the lateral aspect of the arm. You can also test by motor abduction of the deltoid. Films must be obtained prior to reduction if: first time dislocation, age over 40, presence of humeral ecchymosis, or traumatic mechanism. The scapular Y view will demonstrate anterior dislocation of the humeral head from the glenoid. Associated injuries to look for include Hill sachs defect, bankart lesions, fractures of the greater tuberosity, soft tissue injuries, and rotator cuff tears. While we will not discuss in depth associated injuries, it is important to be aware particularly of hill sachs and rotator cuff tears. Hill sachs defect presents in up to 40% of anterior dislocations; this defined by a radiographic defect in the posterior lateral portion of the humeral head. Rotator cuff tears, also common, present more commonly in older patients. It is estimated between 35-86% of anterior dislocations in patients over 40 years old have a rotator cuff tear. Shown below includes image of anterior shoulder dislocation with hill-sachs deformity on the left; and anterior shoulder dislocation with bankart lesion on the right. 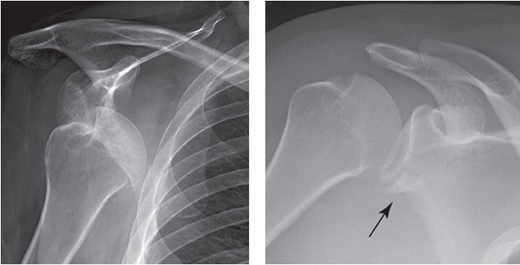 There are several techniques for reduction, none of which have proven more efficient or effective over the other. A common technique, used in this patient, is the external rotation method. Patient sits up, straight back. Examiner holds the elbow at the patients side and with forearm in 90 degree angle, slowly externally rotates the arm. After successfully reduction, the arm is immobilized with splint and post reduction films obtained. Immobilization should be for 3 weeks if younger than 30 yrs old, and for 7-10 days if over 30 yrs old.
1 Comment
|
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
