HPIThis is a 13 yr old Caucasian male with no significant past medical history who is presenting with 2 week history of right hip pain. He describes a vague pain localized around the right hip worsened with movement mostly flexion and extension of the hip. No known alleviating factors. No history of trauma, fever, chills, nausea or vomiting, recent weight loss or night sweats. No other joints involved. No family history of rheumatologic or bone disorders. physical examGeneral: Obese male, laying flat on bed in no distress. RLE: Right lower extremity is slightly externally rotated compared to left. No thigh or calf atrophy. No erythema, swelling, or warmth to touch. No abrasions, lacerations or ecchymosis. 2+ dorsalis pedis pulse. Sensation intact in all dermatomes. Full active range of motion of right hip. Passive range of motion however is significant for slight external rotation with flexion of the hip. No patellar or fibular head tenderness. Full active and passive range of motion of knee. Noted to have slight external rotation of right lower extremity with gait. GU: Normal male genitalia. No erythema, swelling, or tenderness of penis or scrotum. No urethral discharge. LLE: No erythema, swelling, or warmth to touch. No abrasions, lacerations or ecchymosis. 2+ dorsalis pedis pulse. Sensation intact in all dermatomes. Full active and passive range of motion of hip. No patellar or fibular head tenderness. Full active and passive range of motion of knee. radiographs Diagnosis and treatmentIsolated right slipped capital femoral epiphysis. No involvement of the left side. Patient was taken to the operating room the following day and underwent percutaneous in situ fixation with two cannulated screws. TSH and free T4 obtained, normal. Counseling on weight loss provided. discussionSlipped capital femoral epiphysis (SCFE) is a disorder where the femoral epiphysis displaces from the femoral neck through the physeal plate. It is a common hip disorder in adolescents affecting approximately 10 per 100,000. Note however, about 15% will present with no description of hip pain but rather knee or thigh discomfort. Thus it is important to maintain a high degree of suspicion to diagnose and treat early. SCFE is more commonly seen in obese children; obesity is the single greatest risk factor. It more commonly affects males, African Americans, and Pacific islanders. Often it occurs during periods of rapid growth (the average age for boys 13 yrs old, females 12 yrs old). It can be associated with endocrine disorders including hypothyroidism, osteodystrophy of chronic renal failure and growth hormone treatment. If SCFE is diagnosed in a child who is <10 yrs old or whose weight is <50th percentile, an endocrine workup is warranted. The displacement of the epiphysis occurs secondary to mechanical forces. Through the hypertrophic zone of the physis, slippage can occur. Cartilage within the perichondral ring acts as a weak point and with mechanical forces causes displacement. With displacement, the epiphysis remains within the acetabulum. The neck slips anteriorly and rotates externally. The most common presenting complains are pain and altered gait. Classically, an obese child presents with dull pain either in the hip, groin, thigh or knee without any history of trauma. Symptoms can be present anywhere from week to several months. Often an abnormal coxalgic gait is noted. The child may have decreased hip motion with obligatory external rotation during passive flexion of the hip. There may also be abnormal leg alignment with the foot slightly externally rotated and thigh atrophy. Diagnosis is made by radiographs. It is recommended that both an AP and frog-leg lateral of the right and left hip is obtained. 17-50% of SCFE are bilateral. On the AP pelvis, Klein’s line can be drawn to help diagnose. This line is drawn along the superior border of the femoral neck. In a normal hip, the line will intersect the femoral head. In SCFE, Klein’s line does not intersect the femoral head. 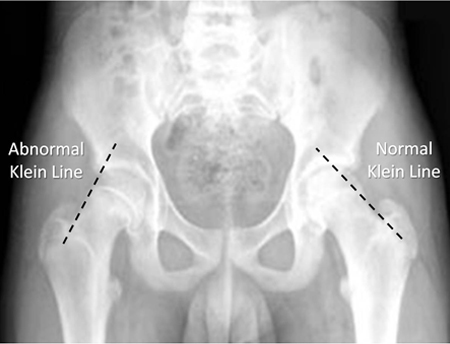 PIf the child is able to ambulate, it is termed stable. Unstable SCFE occur in children unable to ambulate or if the epiphysis is displaced from the metaphysis. Each is treated by making the child non-weightbearing until orthopedic consultation and treatment. The importance in the difference is children with unstable SCFE may have further displacement with any manipulation; thus it is extremely important to immediately place child on stretch and instruct to not ambulate. Children with SCFE should be referred to orthopedics promptly. Non-weightbearing is required until treatment. Treatment is surgical by either percutaneous in situ fixation or open reduction with the capital realignment. pearls1. SCFE is where the femoral epiphysis displaces from the femoral neck
2. More common in obesity, males, African American, and Pacific islanders 3. Can be associated with endocrine disorders 4. Order AP and frog-leg views bilaterally to diagnose, assess Klein's line 5. Urgent orthopedic consultation for surgical treatment
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
