|
HPI: Right hand dominant middle aged female with history of HTN presents to the ED after accidentally hitting her left index finger with a hammer while working on a home improvement project. Finger is painful and swollen but she has no other injuries and reports she is otherwise feeling well. Physical Examination: Erythematous, swollen, and tender left 2nd distal phalanx. There is a subungual hematoma present over approx. 75% of the nail but the nail is intact. Motor and sensation intact, full ROM of PIP and DIP, 2+ radial pulse, no other injuries identified. Radiology: AP, lateral and oblique views of left 2nd phalanx – no fracture or dislocation identified Management: Nail removal and bedside repair of nail bed laceration, tetanus updated, discharged home with 48 hour follow up for reevaluation Discussion: Fingertip injuries = most common hand injuries seen in the ED Most common mechanisms:
Evaluate for:
Complications of injury:
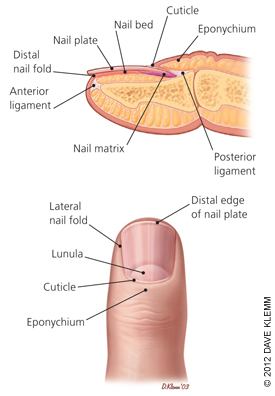 Image obtained from Am Fam Physician. 2012 Apr 15;85(8):779-787. Fingertip Anatomy:
Blood Supply and Innervation:
Nail Growth:
Treatment: Obtain radiographs to rule out distal phalanx fracture Evaluate for subunginal hematoma and nail bed lacerations Drain hematoma if <50% nail involved
Nail removal, I&D, repair of nail bed if >50% of nail involved
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
