|
HPI: 20ish year old and otherwise healthy male presents as the restrained driver in head-on MVC at low speed just prior to arrival. He has a large linear laceration to anterior aspect of R knee and is unable to fully extend the knee. Wound is hemostatic. No other injuries or complaints. Physical Examination: 10cm linear, horizontal laceration to the anterior aspect of the patient’s R knee. Knee is held in slightly flexed positioning. Decreased ROM of the knee secondary to pain and injury, patient unable to actively extend extremity in straight leg raise. FROM of ankle. 2+ DP and PT pulses present. Sensation intact to light touch throughout. No erythema, swelling or significant tenderness present over RLE. Radiology: AP/Lateral/Sunrise/Oblique views of R knee: Transverse fracture of the patella with 3mm of displacement present and surrounding soft tissue edema Management:
Discussion:
Types of fracture:  Figure obtained from jaaos.org; Patellar Fractures in Adults; AAOS April 2011 vol. 19 no. 4 198-207,Figure 4 A) Nondisplaced B) Transverse C) Pole or sleeve (upper or lower) D) Comminuted nondisplaced E) Comminuted displaced F) Vertical G) Osteochondral Evaluate with physical examination first Severe knee pain and soft tissue swelling should raise suspicion for injury Concerning findings:
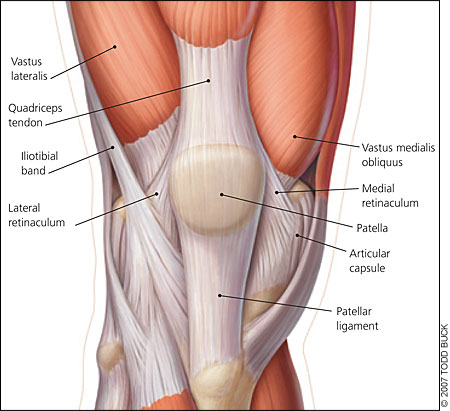 Image obtained from aafp.org, Am Fam Physician. 2007 Jan 15;75(2):194-202. Obtain Radiographs
Fracture displacement best viewed on lateral films, but obtain AP/Lat/Oblique/Sunrise to fully evaluate Degree of displacement = degree of retinacular disruption Treatment: Nonoperative:
Early active ROM with hinged knee brace after 2-3 weeks Operative:
Pearls: Watch out for patella sleeve fractures in peds – need high index of suspicion to diagnose
Bipartite patella = failure of bony fusion
Any lacerations present must be assumed to communicate with the knee joint until this assumption is disproved by a saline load joint challenge A patellar fracture is problematic and requires intervention if extensor mechanism of knee is nonfunctional = unable to perform straight leg raise test
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
