|
HPI: Pediatric male presents after a fall onto outstretched arm with obvious deformity to right elbow. PE: Patient is unable to cross fingers and has paresthesias in the ulnar nerve distribution. Initial radiograph showed posterior dislocation with questionable hyperdensity representing the medial epicondyle. We were unable to reduce under fluoroscopy as the medial epicondyle was more visible and the patient eventually required ORIF. Imaging: AP and lateral radiograph of the elbow 
Image 1: Showing associated medial epicondyle fracture How to Diagnosis: Two important lines help in making the diagnosis; radiocapitella and anterior humeral. Radiocapitellar line: Drawn through the center of the radial neck and should pass the center of the capitellum as shown below 
Anterior humeral line: Drawn through the lateral view of the surface of the humerus and should pass through the middle of the capitellum 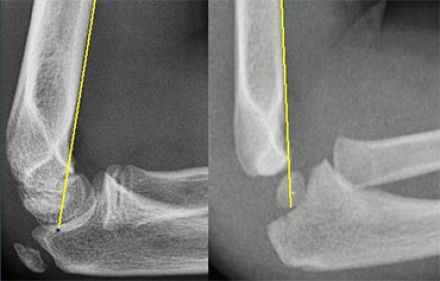
Ossification: 6 sites that fuse at different ages. Mnemonic = CRITOE
Treatment: Nonoperative with closed reduction and early range of motion (1-2 weeks) is most common. ORIF required for incarcerated medial epicondyle, inability to obtain close reduction, or significant instability. Pearls:
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
