|
HPI: An otherwise healthy 39-year-old female presents to the emergency department complaining of right shoulder pain. She had a fall the night previous where she fell directly onto the point of her right shoulder. She had dull, moderate pain but went to sleep after the fall as it was late and she had been drinking. She woke up on the morning of presentation with excruciating shoulder pain, inability to move her arm secondary to pain and a visible of the right shoulder deformity. No other traumatic injuries, no other complaints. She is not able to move her shoulder but can move her elbow and hand okay. No paresthesias, no weakness in the right arm. On physical exam, Her right shoulder is held against body, flexed at elbow. There is exquisite point tenderness over the AC joint. Appears deformed on visualization, with down-sloping of the anterior shoulder. Skin is intact. Palpation of the long bones and hands does not elicit tenderness or crepitus. The clavicle is neither tender nor deformed. Active/passive elbow and wrist range of motion is full and painless. Passive ROM of the right shoulder is not tolerated well secondary to pain. Patient can give a thumbs up, make an okay sign, and cross his index and long fingers without issue. Sensation to light touch is intact in the radial, median, and ulnar nerve distributions in the hand. Radial pulse is palpable. Right shoulder XRs were performed and are shown below. What is the diagnosis? Should you prepare the patient for shoulder reduction? Answer: AC Separation AC separation of the shoulder usually results from direct trauma to the AC joint, when the arm is in an adducted position. Support of the AC joint is through the acromioclavicular and coracoclavicular ligaments. Tenderness and deformity at the AC joint is diagnostic of this clinically. XRs are performed to confirm the diagnosis and also rule out underlying fracture. 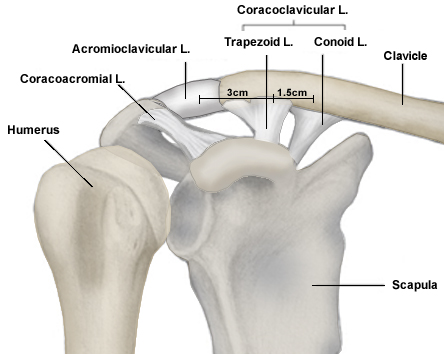 Image Credit: Orthobullets There are six types of AC separation. Involvement of the AC and CC ligaments determine the severity of acromio-clavicular injury. The types increasingly worsening in severity. 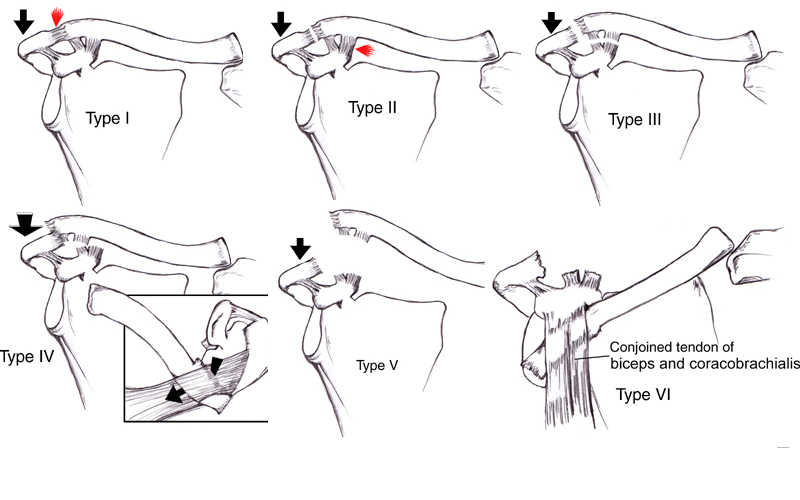 Image Credit: Orthobullets 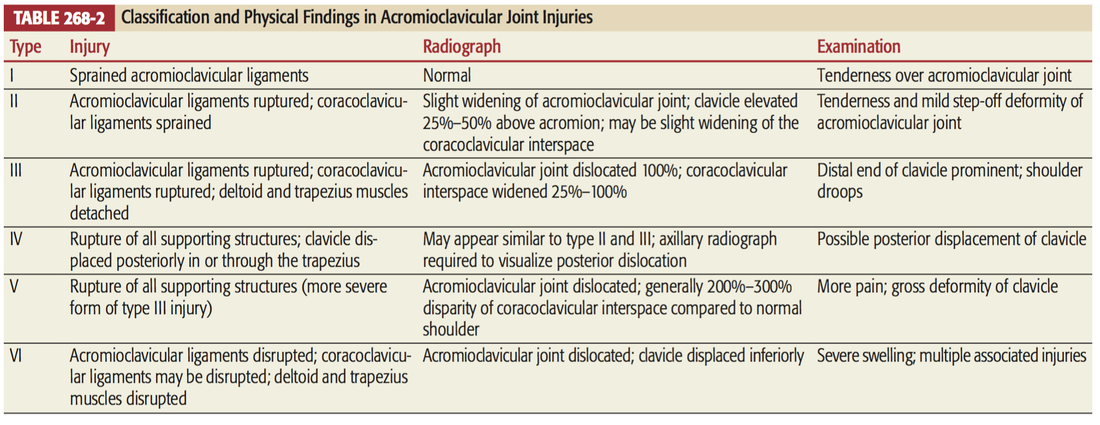 Image credit: Tintinalli's Radiographs: Must have True AP, Axillary and Scapular Y views to diagnose (to rule out associated dislocation or fracture).  Image Credit: Orthobullets The normal AC joint space is 3mm and the normal coracoclavicular distance is 13 mm. Anything larger than these are pathologic. 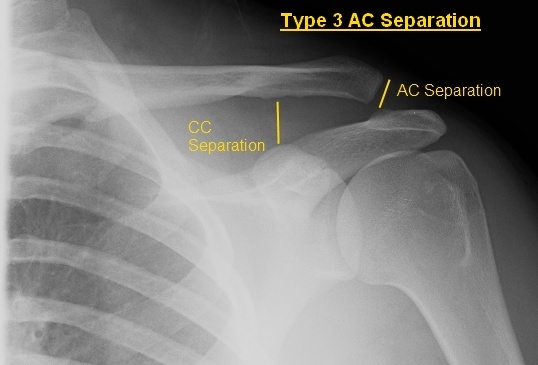 Image courtesy of: http://ortho-teaching.feinberg.northwestern.edu/cases/shoulder/case8/diagnosis.html%E2%80%8B Management:
Treatment of type I and II injuries consists of rest, ice, analgesics, and immobilization (sling), followed by early range-of-motion exercises (7 to 14 days). Orthopedic consultation for Types III through VI. Operative management is ORIF or ligament reconstruction: Type III in elite athletes, Types IV-VI. By: Dr. Michael Mollo M.D. References: 1. Rudzinski J Pittman L Uehara D: Injuries to Bones and Joints, in Tintinalli J., et al (eds): Tintinallis Emergency Medicine: A Comprehensive Study Guide, ed 7., (Sec) 22 (Ch) 268:p 1832-1834. 2. Orthobullets 3. Northwestern Orthopedics
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Orthopedics Blog
AuthorCMC ER Residents Archives
June 2018
Categories
All
Disclaimer: All images and x-rays included on this blog are the sole property of CMC EM Residency and cannot be used or reproduced without written permission. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the author and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
