
Use the appropriate order set for all "Code" patients!
0 Comments
 • If even considering CVA as diagnosis, call Code Stroke
• Consider mechanical thrombectomy in CVA patients who may not be IV tPA patients • Role of head trauma in IV tPA exclusion criteria poorly defined • Always consider VTE in pregnant patients with leg pain • Pregnant & postpartum patients are at significantly increased risk of VTE • Diagnostic workup with Modified Well’s Criteria • Lovenox is the treatment of choice for VTE in pregnancy 
 Psychiatric and medical co-morbidities
ERIC forms
Restraints
 Case 1:
Case 2:
Case 3:
 Define status epilepticus:
Consider etiologies:
Remember ABCs and supportive care in addition to treating seizures Learn dosing for hypoglycemic seizure with dextrose
Learn dosing for hyponatremia seizure with 3% NaCl Medications First line:
Second line:
Refractory/Third line:
 Naloxone:
Cocaine:
Heroin:
 General 1. WCT algorithms do not work in the real life setting 2. Don’t pay attention to what others have said; you need to evaluate the ECG yourself 3. First question: is the WCT regular or irregular? Sustained Regular WCT I. Differential Diagnosis 1. Sustained regular WCT: most likely ventricular tachycardia (VT) a. Spend 2 minutes searching for P waves – inconsistent P-QRS relationship is 100% specific for VT b. Bizarre QRS morphology that is not c/w RBBB or LBBB (negative QRS in lead I; QRS concordance in the chest leads) strongly supports VT 2. Consider SVT if QRS morphology resembles RBBB or LBBB a. Find an old ECG: are the QRS morphologies identical? b. If no old ECG available, prove SVT by giving IV adenosine c. “I think this is SVT” is not good enough! II. Therapy of Sustained Ventricular Tachycardia 1. Unstable: electric cardioversion 2. Clinically stable: one round of IV antiarrhythmic drug therapy allowed a. IV procainamide may be the most effective agent (avoid in patients with severe systolic CHF and in patients with baseline prolonged QT) b. IV amiodarone c. Consider IV propranolol or IV metoprolol in ischemic VT and in patients with “electric storm” (repeat episodes of VT/VF) Sustained Irregular WCT I. Differential Diagnosis 1. Sustained irregular WCT: most likely not VT but atrial fibrillation (AF) 2. Rate 120-160; QRS morphology is c/w RBBB or LBBB: AF with bundle branch block 3. Rate very fast; QRS morphology is bizarre, not c/w RBBB or LBBB: most likely AF with WPW (FBI – Fast, Broad-complex, Irregular) II. Therapy 1. AF with BBB: usual therapy for AF (IV diltiazem etc.) 2. AF with WPW (“FBI”) a. Clinically unstable or ventricular rate excessive: electric cardioversion b. Clinically stable: IV procainamide or IV ibutilide c. Clinically very stable, rate not very fast: PO flecainide or propafenone NOT ALLOWED: IV verapamil, diltiazem, digoxin, adenosine 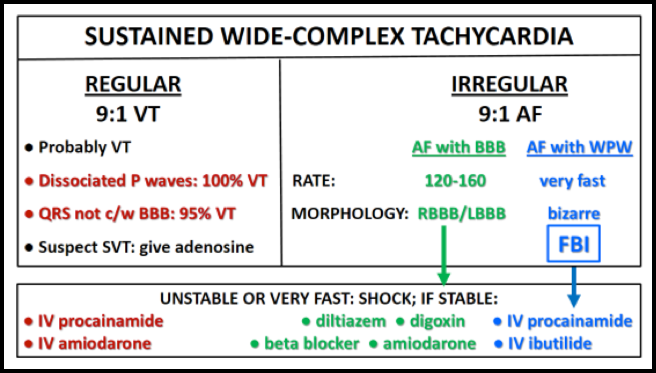  The mnemonic for systematically evaluating a non-contrast head CT is “Blood Can Be Very, Very Bad”.
A Reassuring CT: · No Blood is seen · All Cisterns are present and open · Brain is symmetric with normal gray-white differentiation · Ventricles are symmetric without dilation · No hyperdense Vessels are present · No Bone fractures  1. Four recently completed trials demonstrate that early mechanical stent-thrombectomy after tPA in patients with large vessel occlusion and salvageable tissue on brain imaging results in improved reperfusion and functional outcomes.
2. The details of the patient selection paradigm remain a key discussion, but favorable penumbral imaging is a consistent feature of all trials. 3. Systems of acute care, including transfer protocols, will need to be re-organized to deliver this therapy effectively in the real world |
Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed
