
0 Comments
 -- Despite your location in the ER, treat all 'in extremis' patients with the same approach:
ABCs, reversible causes (glucose, narcan, epi), resuscitate patient and then move to higher care area -- Contrast reactions cause an anaphylactoid reaction, which is treated with same supportive measures as an allergic reaction (epi, steroids, antihistamines) -- There are almost no contraindications to receiving contrast (the shaky area is with CKD or patients with AKI) - be sure to hydrate patients before and after scans if they can tolerate it -- Only need to order irradiated or CMV negative blood products for patients with leukemia/lymphoma or transplant patients -- Order Type and Screen (rather than T&C) on patients unless they need to be transfused in the ED/imminently. -- You can order MTP on patient as soon as they are registered; however, keep cooler closed until you definitively know you will need to transfuse - Always think inside AND outside the abdomen when evaluating children for abdominal pain
- Obstruction in children does not always produce distension or peritoneal signs - To accurately evaluate for obstruction you need supine and upright (or decubitus) Xrays - Lethargy can be the sole presentation of intussusception in infants and toddlers (See PedEMMorsel) - Bilious emesis in neonates is a surgical emergency even if they look well - Pyloric stenosis rarely occurs after 8-10 weeks of age  High ETOH concentration is protective against methanol and ethylene glycol (metabolized slower as ethanol is metabolized first) Ethylene Glycol - the metabolites, not ethylene glycol, cause acidosis and toxicity - ethylene glycol itself, not the toxic metabolites, cause increased osmolal gap - Fomepizole recommended Methanol - Permanent blindness has occurred after ingestion of approximately 1 teaspoon of methanol - Fomepizole recommended Isopropyl Alcohol - Since the parent compound causes toxicity, not the metabolite (acetone), fomepizole not indicated. - Urine ketones will be positive (Ketosis without acidosis) 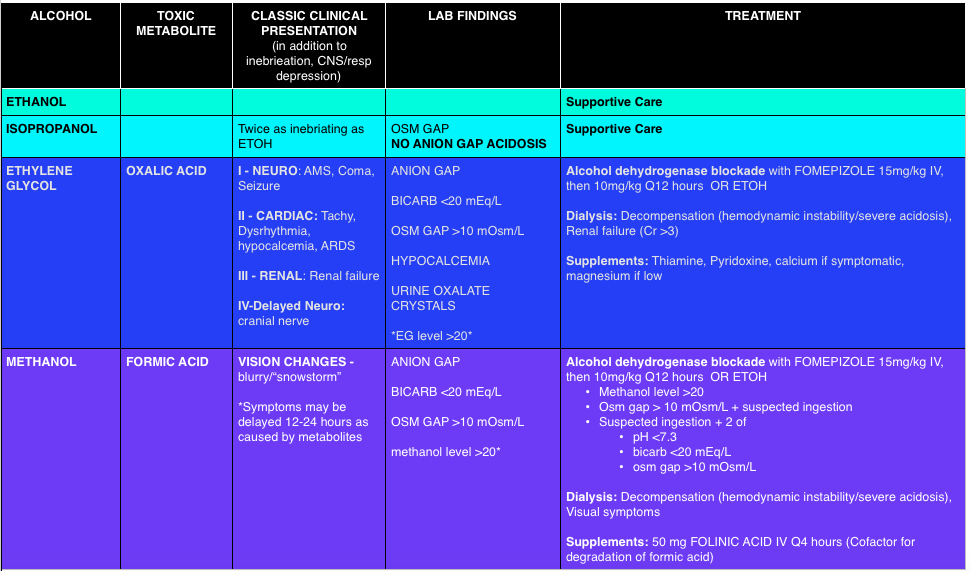 Photo credit: foamcast.org 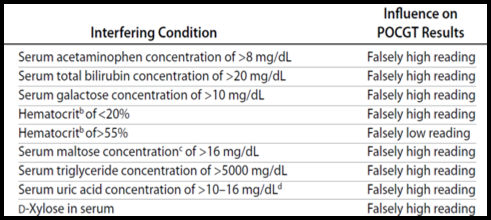 Definition of hypoglycemia:
Interferences with Point of Care Glucose Testing:
Important Toxicologic Considerations:
Glimepiride Glyburide Chlorpropamide Tolbutamide Tolazamide
Nateglide Repaglinide Similar action to sulfonylureas but shorter duration of action. Ethanol:
Dulaglutide (Trulicity®) Exenatide (Byetta,Bydureon®) Liraglutide (Victoza®) Amylin analogue: Do not cause hypoglycemia Pramlintide (Symlin®) Antidiabetic drugs that are expected to cause hypoglycemia
Normoglycemic Ketoacidosis:
 Cat Scratch Disease:
Toxoplasmosis
Bites:
Toxocariasis:
|
Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed
