 - Hypothermia: Can cause significant physiologic disturbance, generally starting when body temperatures fall beneath 90 degrees (moderate hypothermia). Moderate hypothermia should be aggressively corrected with both external and internal warming measures. Risk of refractory VFIB increases as you approach 82.4degrees.
- Severe hypothermia requires invasive rewarming techniques including invasive catheters (think therapeutic hypothermia in reverse). This can include hemodialysis and ECMO. - Peri-intubation hypothermia: associated with increased risk of mortality as well as increased ICU and hospital length of stay. Take steps to avoid it! Think ketamine, fluids, pressors. - Spinal shock: sudden vasoplegia caused by loss of output from sympathetic system. Classic presentation of hypotension and bradycardia is seen in less than 25% of cases. Most recent guidelines recommend norepinephrine as pressor of choice. Seen mostly commonly in injuries above T6.
0 Comments


 1. Use of CTP imaging to determine eligibility for revascularization therapy is unproven in randomized studies.
2. Appropriately performed PCT performs reasonably well at identifying core acute infarct associated with large vessel ischemic strokes. 3. PCT unproven in distinguishing penumbra from benign oligemia. 4. Further standardization and validation of PCT needed.  Case 1: Missed appendicitis
1. Appendicitis in children less than 3 years of age: a 28-year review. Pediatr Surg Int. 2004 Jan;19(12):777-9. Epub 2004 Jan 16. 2. Acute appendicitis in children under 3 years of age. Diagnostic and therapeutic problems. Med Wieku Rozwoj. 2012 Apr-Jun;16(2):154-61. 3. The presentation of appendicitis in preadolescent children. Pediatr Emerg Care. 2007 Dec;23(12):849-55. 4. Pain as the only consistent sign of acute appendicitis: lack of inflammatory signs does not exclude the diagnosis. World J Surg. 2010 Feb;34(2):210-5. doi: 10.1007/s00268-009-0349-z. Case 2: Tako-Tsubo Cardiomyopathy and Hypertensive Emergency
Case 3: Incidentalomas
Case 4: Sporotrichosis
 Soft tissue Ultrasound:
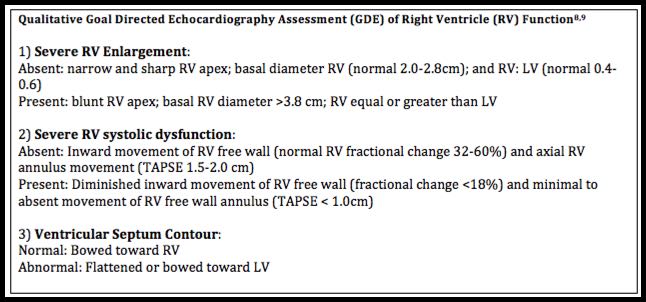
Echocardiography Tips: Eyeball qualitative LV systolic function assessment: -mitral annulus movement along the long/major axis -LV wall movement inward along minor axis -thickening of LV wall during systole -proximity of anterior leaflet of MV and septal wall Eyeball qualitative RV assessment: - RV tends to dilate before it goes bad (with acute pulmonary embolism physiology) - RV shape and function more complex - Most significant movements of RV are along long/major axis [NERD alert!: TAPSE (tricuspid annular planar systolic excursion)] Image Acquisition Tips: - Focused RV assessment: - Apical window: angle medially toward RV to get better view of RV apex, free wall and annulus - Use subcostal window… must view RV apex - Parasternal long: angle anteriorly and you’ll see both RV & RA - Looking for RV enlargement (RVE): - Look for RVE Apex enlargement + widened RV base - Subcostal and apical views to get a good look at the apex - Parasternal short axis view - Normal contour of RV semilunar/croissant next to donut (LV) - RVE might show as ‘helmet’ rather than ‘croissant’ Tips to Avoid Trips
Aggressive treatment of cyanide
When to pursue HBO for carbon monoxide Think of this in pts with LOC, cerebellar symptoms, persistent HA after 4 hrs of supplemental oxygen |
Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed
