 1) Use both EKG and absolute K value, in addition to clinical picture, to determine necessity for treatment of hyperkalemic emergency 2) Suspect HyperK in any renal patient who presents with arrhythmia, and correct before pursuing other interventions 3) Be aware of onset times and half-life of HyperK treatment meds (Ca, insulin, B-agonists), and redose as needed! 4) Glucose checks q30min or q1h in any patient treated with insulin for HyperK 5) "C BIG K Di" mnemonic (Calcium, bicarb/Beta agonist/Insulin/Glucose, Kayexelate/LasiKs, DIalysis) 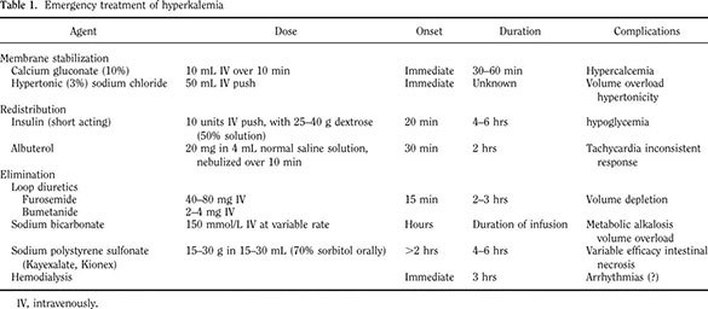
0 Comments
 ARSENIC
MERCURY
LEAD
Remember that metals are caustics.  1) "The brownie on eights are tricky" - translated to febrile neonates are tricky - must remain vigilant!
2) knowledge is important, but we must recognize limitations (regarding studies, gray areas, etc.) 3) scheduled and ensured hospital follow-up is essential! |
Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed
