 I. Characteristics of respiratory artifact
II. The clinical significance of respiratory artifact
III. Respiratory artifact can aid in the recognition of sleep-disordered breathing
b. an abrupt increase in heart rate and the c. simultaneous appearance of very fast RA
b. simultaneously occurring very long respiratory (snoring) artifact followed by c. a sudden increase in the heart rate and resolution of the RA
b. the onset of most periods which contain the RAs show the characteristics of central sleep apnea
0 Comments
 What is STEMI without STE?
Posterolateral or High Posterior MI
High Lateral MI
RV infarct
 Differential Diagnosis
When the intrinsic rhythm is sinus: I. What was the first beat of the tachycardia?
When the intrinsic rhythm is atrial fibrillation:
Artifact Always consider artifact if:
 General 1. WCT algorithms do not work in the real life setting 2. Don’t pay attention to what others have said; you need to evaluate the ECG yourself 3. First question: is the WCT regular or irregular? Sustained Regular WCT I. Differential Diagnosis 1. Sustained regular WCT: most likely ventricular tachycardia (VT) a. Spend 2 minutes searching for P waves – inconsistent P-QRS relationship is 100% specific for VT b. Bizarre QRS morphology that is not c/w RBBB or LBBB (negative QRS in lead I; QRS concordance in the chest leads) strongly supports VT 2. Consider SVT if QRS morphology resembles RBBB or LBBB a. Find an old ECG: are the QRS morphologies identical? b. If no old ECG available, prove SVT by giving IV adenosine c. “I think this is SVT” is not good enough! II. Therapy of Sustained Ventricular Tachycardia 1. Unstable: electric cardioversion 2. Clinically stable: one round of IV antiarrhythmic drug therapy allowed a. IV procainamide may be the most effective agent (avoid in patients with severe systolic CHF and in patients with baseline prolonged QT) b. IV amiodarone c. Consider IV propranolol or IV metoprolol in ischemic VT and in patients with “electric storm” (repeat episodes of VT/VF) Sustained Irregular WCT I. Differential Diagnosis 1. Sustained irregular WCT: most likely not VT but atrial fibrillation (AF) 2. Rate 120-160; QRS morphology is c/w RBBB or LBBB: AF with bundle branch block 3. Rate very fast; QRS morphology is bizarre, not c/w RBBB or LBBB: most likely AF with WPW (FBI – Fast, Broad-complex, Irregular) II. Therapy 1. AF with BBB: usual therapy for AF (IV diltiazem etc.) 2. AF with WPW (“FBI”) a. Clinically unstable or ventricular rate excessive: electric cardioversion b. Clinically stable: IV procainamide or IV ibutilide c. Clinically very stable, rate not very fast: PO flecainide or propafenone NOT ALLOWED: IV verapamil, diltiazem, digoxin, adenosine 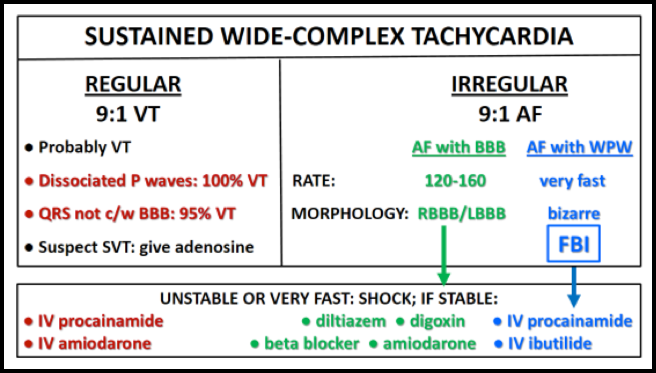 Bifascicular Block and Second Degree AV Block1. In asymptomatic individuals, chronic bifascicular block does not usually require cardiac work-up; the prognosis is generally benign 2. The following high-risk features, however, warrant urgent evaluation: a. Bifascicular block and syncope b. Bifascicular block and intermittent second degree AV block c. 1:1 AV conduction at slower sinus rates but higher grade block (i.e., 2:1 AV conduction) at faster sinus rates (“acceleration-dependent AV block”) 3. Evaluation and management of patients with bifascicular block: a. Actively search for nonconducted P waves in the 12-lead ECG b. Always review telemetry strips and actively search for episodes of second degree AV block (blocked P waves) c. In symptomatic patients with bifascicular block who develop acceleration-dependent second degree AV block and a very slow ventricular rate, carotid massage or IV beta blocker can paradoxically restore 1:1 AV conduction d. Patients with bifascicular block and syncope require admission and cardiology consultation for possible pacemaker implantation e. Patients with bifascicular block and intermittent second degree AV block require cardiology consultation for possible pacemaker implantation The Pacemaker ECG1. Ventricular pacing: always try to determine what the atria are doing
2. Sinus P wave in front of each paced QRS complex indicates dual chamber (A-V sequential) pacemaker where the ventricular pacer is tracking sinus rhythm 3. Two pacer spikes about 5 mm apart indicate AV sequential pacing 4. If there are no P waves or 2 pacer spikes, search for the presence of retrograde P waves after the paced QRS complexes; retrograde P waves are sharp negative in the inferior leads (in II, III and aVF) and usually upright in V1 5. If there are no P waves in front of the paced QRS complexes and no retrograde P waves present, always consider the possibility of underlying atrial fibrillation |
Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed
