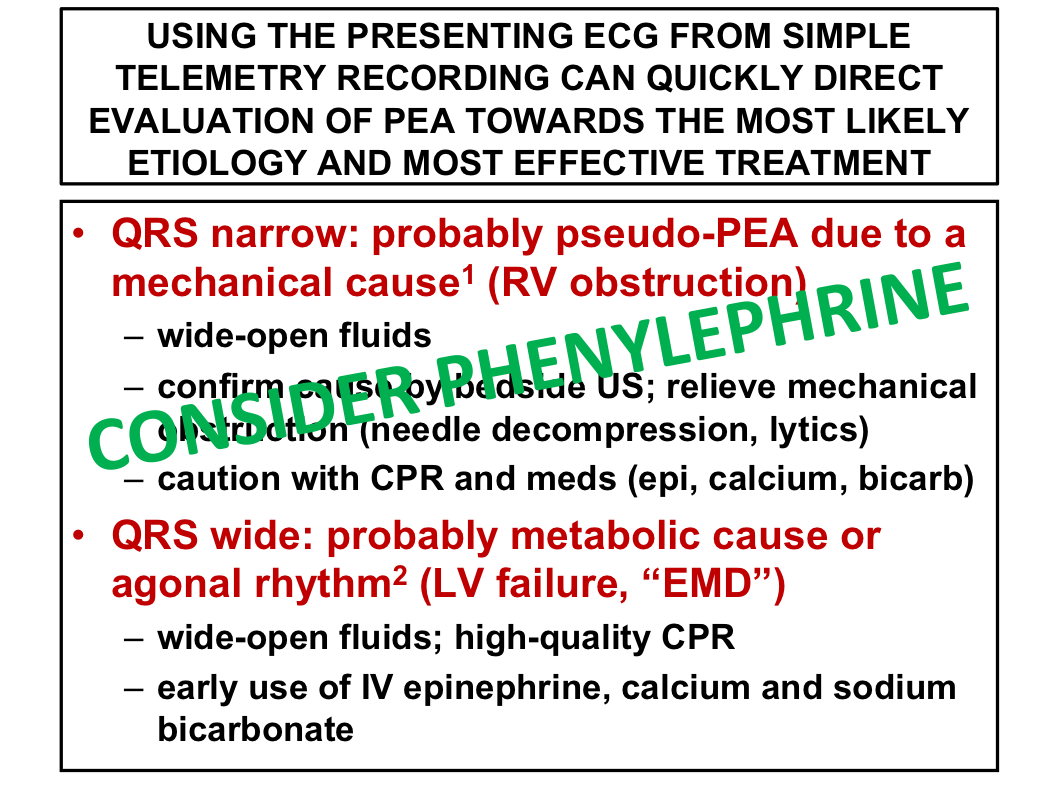
  1. Most common “mechanical” causes:
2. Most common “metabolic” causes:

 1. Several types of angioedema
2. Each has a different treatment
3. Airway and hemodynamic management is critical
4. Cricothyrotomy
 Working in a pediatric ED isn't just diagnosing viruses - child abuse/neglect is more prevalent than we'd like to think:
Providers should be mindful of sentinel injuries - injuries without a plausible explanation
Skeletal injuries are the second most common presentation of abuse - certain fractures should raise your suspicion for abuse
Abusive head trauma (formally known as “shaken baby syndrome”)
Chest and abdominal injuries
What can you do to help prevent a missed diagnosis of abuse?
 Large MCA Strokes
* Although headache is less common in ischemic stroke, the presentation may be deceiving. Some patients with large vessel occlusion will mimic signs of hemorrhagic stroke--headache, vomiting, hypertension, altered mental status. * Irrespective of the 6-hour window or 3 hour post wake up window, consider paging out a code stroke if you're concerned or hedging. Thrombectomy is to be considered! * Time is brain. Data suggests there is likely a direct correlation between speed of treatment and better outcomes, particularly with endovascular data. * Neurons over nephrons? When considering contrast burden of CT perfusion studies, consider the devastating effects of the stroke vs potential kidney damage * Data on IV tPA may be controversial but the endovascular/thrombectomy data suggests a NNT of as low as 4 patients! This could be the way of the future for stroke care. * tPA is likely okay with carotid dissection. tPA is NOT okay with aortic dissection * Aortic dissection would affect R hemisphere but would be rare and quite unlikely to cause solely L hemispheric deficits Unstable Junctional Bradycardia * Junctional rhythm with unstable bradycardia? Think about drugs before the need for transvenous pacemaker * Severe digitalis toxicity can rarely result in temporary cessation of atrial fibrillation and the appearance of a slow junctional rhythm without P waves. Occasionally, when the digitalis toxicity improves, the atrial fibrillation returns * Hyperkalemia, essentially a Na channel blocker, should be considered with all junctional rhythms * We don't always perform medication reconciliation but an argument could be made that looking at the drug list tells you more about the PMH and PSH than perusing the record Central line trouble shooting: -- do not force the guide wire -- do not re-use a bent guide wire -- use your ultrasound to confirm placement with modified bubble study -- consider chest x-ray while still sterile to gauge line placement Modified bubble study for confirming central line placement: 1. Obtain US view of the RA/RV 2. Shake up a flush (without adding air) 3. Rapidly push flush through one of the ports 4. Should see dynamic echogenicity within the RA/RV if venous access  1. HSV Encephalitis has significant morbidity and mortality, during your history ask about Maternal AND Paternal history of HSV.
2. You should cover for HSV meningitis with acyclovir when:
4. Signs of traumatic aortic injury include:

|
Archives
August 2018
Categories
All
|

 RSS Feed
RSS Feed
