0 Comments
 Dr. Allen Dr. Allen Definition:
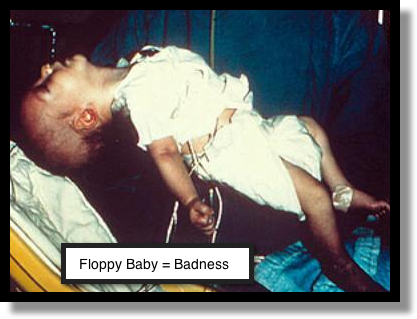 Infantile Botulism Infantile Botulism
16 yo with syncope 16 yo who passed out on airplane with lots of social stressors.
13 yo with abdominal pain "Chronic" abdominal pain over past 2-3 months.
Always beware of diagnostic momentum!
Young age alone does NOT rule out ACS Very Low risk patients are defined and may be D/C'd with no further ED evaluation
Non-specific ST changes are NOT negligible in the symptomatic patient. PITFALL: Placing too much emphasis on "atypical" symptoms for ACS Things that Increase Likelihood Ratio for ACS/MI
NO Studies risk-stratify patients to NO risk. Characteristics of pts D/C'd with missed MI
Know your ECGs! You need to strive to be the ECG Master in your hospital! So invest some time and effort into it... Learn from the best: http://www.mededmasters.com/ecg-lessons-by-amal-mattu.html
Basics
NEXUS Criteria for Chest Imaging see article (http://archsurg.jamanetwork.com/article.aspx?articleid=1724982) see review (http://www.2minutemedicine.com/nexus-chest-decision-criteria-sensitive-for-thoracic-injury/) Tells you who does not need chest imaging. If the patients LACKS the following, then you do not need chest imaging:
PTX
Traumatic Aortic Injury
Rib Fx

Complications of Zoster
Indications for Treatment
Medical Management
Pediatric myocarditis Background
SOCIAL HISTORY What counts as a social history: a lot!
It can be obtained from HPI (ex, 63 yo sent from Skilled Nursing facility... or, 4 yo who fell at Pre-School... all of that counts). Case 1 - 61 year old with Rapid Heart Rate
Case 2 - 30 year old with abdominal and rectal pain
Case 3 - 63 year old with dyspnea and uri symptoms
|
Archives
August 2018
Categories
All
|


 RSS Feed
RSS Feed
