 http://www.aafp.org/afp/2003/0201/p537.html http://www.aafp.org/afp/2003/0201/p537.html Geriatric Pts aren't Old Adults
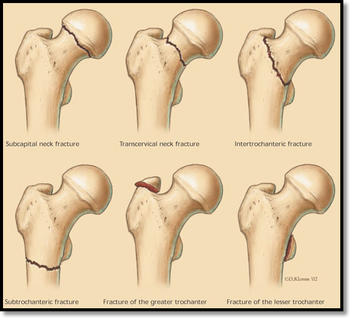
- Fractures can occur with Low energy! - Two anatomical location - Femoral neck (blood supply threatened if displaced) - Intertrochanteric ( capsule instertion) X-rays needed for operative planning - Ap pelvis, AP and lat ofhip, femur, knee Occult Fx - MRI > CT, but CT is still much better than X-ray. Fragility Fx - Needs medical consult - Improves operative outcome. - Fragility fracture orderset required for Medicare payment! How to Classify - Open, Displaced, Comminuted (all yes/no questions) - Displaced = unstable and hip replacement (total vs hemiarthroolasty depends on functional status) - Non-displaced / stable (vagus deform)= screws - Low rates of AVN, Infection, Out Of Bed quickly Outcomes - Mortality - 25% 1 yr mortality - Function - you lose some fuctional status active vs community walker vs house walker vs bed bound
0 Comments
 Pathophysiology
Based on 2 concepts - Increased hydrostatic pressure - Decreased oncotic pressure CXR - Upright films will detect effusions >400mL - Lateral decubitus films will detect as little as 50mL of fluid Fluid analysis - Order: cell count, gram stain, culture, pH, protein, LDH Exudate vs transudate - use Light's Criteria Transudates: CHF Nephritis Nephrotic syndrome Exudates: Infection Traumatic HTX Malignancy CT disorders Management: - Treat the underlying pathology! - Avoid large volume taps (>1L) if CHF, renal or hepatic pathology - Unstable - septic shock, tension hydropneumothorax - If tapping: - Avoid NV bundle - Have patient lean over table - Use ultrasound - When to tap: - Typically, these patients will not need a tap or tube in the ED. - If patients have persistent hypoxia in spite of other interventions, consider tap. - Severe respiratory failure. Complications: PTX Infection Hemorrhage Rare - air embolism, sheared catheter loss  Kids are Different
- Larger heads, tongues, smaller nostrils - Cricoid ring determines size of ET tube - Bradycardia is a BAD SIGN. Signs of Increased Respiratory Effort - Assumed position - Bobbing head - If kids are pulling off their mask, they might need to be intubated. Positioning - sniffing position, sometimes achieved without any padding - jaw thrust is preferred to chin tilt - always use an oral airway, measure from angle of mouth to angle of jaw DOPE for ETT problems - Check ETCO2 waveform - Dislodged - Occluded - PTX - Equipment Pitfalls Not recognizing compromise early! Not thinking to clean out the nose! Not thinking in terms of axis alignment!  Timing Matters
1. Single episode - concerning for impending airway compromise - get help! a. Febrile? - tonsills, abscess, mono, croup, tracheitis, epiglottitis, bronchiolitis b. Afebrile? - airway foreign body 2. Recurrent a. Inspiration - obstruction is above the level of the vocal cords; - Ex, laryngomalacia - from bith; worse with supine. eating or upset b. Expiration - below the vocal cords; - Ex, tracheomalacia in hypotonic kids; vascular anomalies c. Biphasic - at the level of the cords (or just below) - Ex, subglottic stenosis/ hemangioma (get bigger over the first year of life before they start to shrink); vocal cord dyfunction; esophageal foreign body  The Return ED Visit
"BB" Shot to Right Groin...
- Bullet embolism is extremely rare. - Requires multidisciplinary management. - Consider possibility if missile lays next to major vessels or bullets are found in unexpected locations. - Venous more common than arterial FLU 1st presentation - viral symptoms. 2nd presentation - viral symptoms. 3rd presentation (within 24 hours) - SHOCK with Resp Failure
Tamiflu is not magic...
 TRAUMA PATIENTS
- CT if there is abdominal tenderness or a seatbelt sign - Seatbelt sign- Not just abrasions! They have bruising / ecchymoses. - With Seat Belt Sign, incidence of hollow viscus injuries (17%); splenic injuries (10%) - Things that are easy to miss on CT scan - Diaphragm injuries - think about in abdominal pain w/ dyspnea or chest pain - GI tract injuries - free fluid; bowel in discontinuity - Pancreatic injuries - difficult to tell difference between contusion and ductal injury - - Important because these need intervention and waiting will be detrimental; - ERCP or MRCP - definitive diagnosis ABDOMINAL PAIN IN THE ELDERLY - Have a low threshold for imaging elderly patients with abdominal pain - Abdominal pain in elderly - 60-70% admitted; 30% with surgical process; 10% with return ED visits; 5% mortality - Exam is not as reliable!! - CT: diagnostic in 85% of people who had emergent surgical process - Contrast? IV/ PO/ both/ CTA?- if concerned about vascular - get CTA > Contrast allergy - only true contraindication - airway compromise > CIN - Cr rising >0.5 mg/dL or 25% from baseline; > Most elderly people have risk factors Cr > 1.5-2.0 > Consider no contrast - if giving contrast - HYDRATE - Metformin > Manufacture warning - no metformin 48 hrs before or after IV contrast; > Increased risk - contraindications to metfomin, preexisting renal dysfunction BOWEL OBSTRUCTION - Diagnosis - Dilated loops of small bowel - diameter > 2.5 cm; - >50% difference in caliber before and after transition - Acute Obstruction Series X-rays - help if diagnostic; not so much if "normal" or "non-specific" - If an obstruction series is nondiagnostic and you suspect bowel obstruction, get a CT - PO contrast may add functional info, but often difficult to get into the patient... and not necessary. - PO contrast is almost never needed in CT scanning OTHERS - Diverticulitis - fat stranding; bowel wall thickening - CT with IV contrast best image - Appenditicits - senstivity 90% with no contrast; 100% with contrast - Mesenteric ischemia - CT angio is the best - Acute cholecystitis - cholesterol vs pigment stones can be seen on CT - Ultrasound is the first best test for suspected gallbladder pathology - Pancreatitis - Generally don't need imaging. - Consider imaging if changing clinical picture; not typical; no classic pancreatitis risk factors (to r/o malignancy) |
Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed
