 General 1. WCT algorithms do not work in the real life setting 2. Don’t pay attention to what others have said; you need to evaluate the ECG yourself 3. First question: is the WCT regular or irregular? Sustained Regular WCT I. Differential Diagnosis 1. Sustained regular WCT: most likely ventricular tachycardia (VT) a. Spend 2 minutes searching for P waves – inconsistent P-QRS relationship is 100% specific for VT b. Bizarre QRS morphology that is not c/w RBBB or LBBB (negative QRS in lead I; QRS concordance in the chest leads) strongly supports VT 2. Consider SVT if QRS morphology resembles RBBB or LBBB a. Find an old ECG: are the QRS morphologies identical? b. If no old ECG available, prove SVT by giving IV adenosine c. “I think this is SVT” is not good enough! II. Therapy of Sustained Ventricular Tachycardia 1. Unstable: electric cardioversion 2. Clinically stable: one round of IV antiarrhythmic drug therapy allowed a. IV procainamide may be the most effective agent (avoid in patients with severe systolic CHF and in patients with baseline prolonged QT) b. IV amiodarone c. Consider IV propranolol or IV metoprolol in ischemic VT and in patients with “electric storm” (repeat episodes of VT/VF) Sustained Irregular WCT I. Differential Diagnosis 1. Sustained irregular WCT: most likely not VT but atrial fibrillation (AF) 2. Rate 120-160; QRS morphology is c/w RBBB or LBBB: AF with bundle branch block 3. Rate very fast; QRS morphology is bizarre, not c/w RBBB or LBBB: most likely AF with WPW (FBI – Fast, Broad-complex, Irregular) II. Therapy 1. AF with BBB: usual therapy for AF (IV diltiazem etc.) 2. AF with WPW (“FBI”) a. Clinically unstable or ventricular rate excessive: electric cardioversion b. Clinically stable: IV procainamide or IV ibutilide c. Clinically very stable, rate not very fast: PO flecainide or propafenone NOT ALLOWED: IV verapamil, diltiazem, digoxin, adenosine 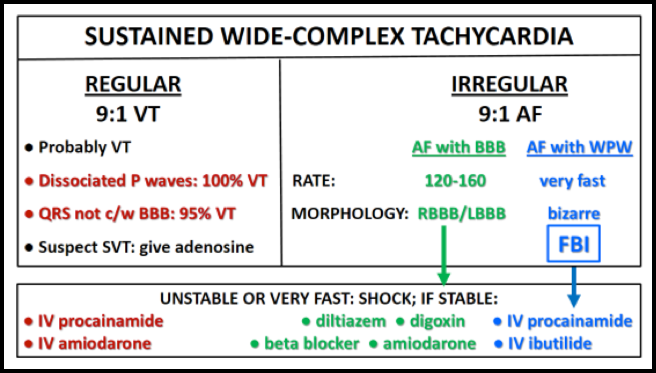
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed
