 Trauma Resuscitation: Not ACLS
It's Not Always Sepsis!
0 Comments


 General 1. WCT algorithms do not work in the real life setting 2. Don’t pay attention to what others have said; you need to evaluate the ECG yourself 3. First question: is the WCT regular or irregular? Sustained Regular WCT I. Differential Diagnosis 1. Sustained regular WCT: most likely ventricular tachycardia (VT) a. Spend 2 minutes searching for P waves – inconsistent P-QRS relationship is 100% specific for VT b. Bizarre QRS morphology that is not c/w RBBB or LBBB (negative QRS in lead I; QRS concordance in the chest leads) strongly supports VT 2. Consider SVT if QRS morphology resembles RBBB or LBBB a. Find an old ECG: are the QRS morphologies identical? b. If no old ECG available, prove SVT by giving IV adenosine c. “I think this is SVT” is not good enough! II. Therapy of Sustained Ventricular Tachycardia 1. Unstable: electric cardioversion 2. Clinically stable: one round of IV antiarrhythmic drug therapy allowed a. IV procainamide may be the most effective agent (avoid in patients with severe systolic CHF and in patients with baseline prolonged QT) b. IV amiodarone c. Consider IV propranolol or IV metoprolol in ischemic VT and in patients with “electric storm” (repeat episodes of VT/VF) Sustained Irregular WCT I. Differential Diagnosis 1. Sustained irregular WCT: most likely not VT but atrial fibrillation (AF) 2. Rate 120-160; QRS morphology is c/w RBBB or LBBB: AF with bundle branch block 3. Rate very fast; QRS morphology is bizarre, not c/w RBBB or LBBB: most likely AF with WPW (FBI – Fast, Broad-complex, Irregular) II. Therapy 1. AF with BBB: usual therapy for AF (IV diltiazem etc.) 2. AF with WPW (“FBI”) a. Clinically unstable or ventricular rate excessive: electric cardioversion b. Clinically stable: IV procainamide or IV ibutilide c. Clinically very stable, rate not very fast: PO flecainide or propafenone NOT ALLOWED: IV verapamil, diltiazem, digoxin, adenosine 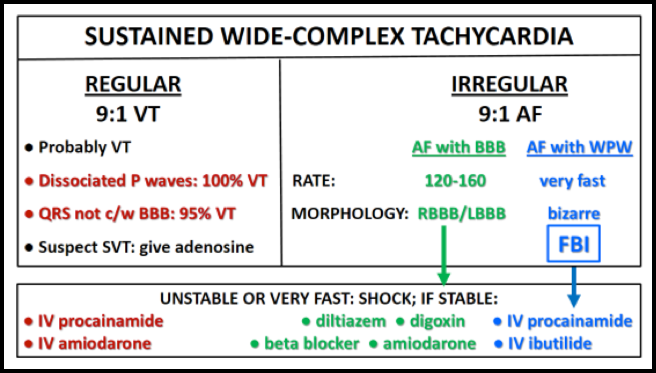  - Respect the anatomic and physiologic differences that exist between adults and kids.
- Focus on the basics! - Compressions >100/min, Good Depth, Good Recoil - Don’t hyperventilate. - EtCO2 can be a helpful guide. - Have a Post-Arrest System in place... at the end of an arrest is not the time to try to figure this out. - Temperature management - ECMO? - Ask the hard questions to help other family members. - Prior syncopal events? - Prior “seizures?” - Prior Submersion Events? - Fam Hx of Sudden Death? - Fam Hx of Submersion Events?  Ovarian Torsion - Ovarian Torsion requires us to be vigilant. It is often misdiagnosed initially by both EM and GYN physicians. - Reconsider your DDx. "Appendicitis" and "Renal Colic" are common mimics of Ovarian Torsion. - Fight diagnostic momentum. - Don’t be fooled by “normal blood flow.” The ovary has two arterial supplies. Diminished venous flow should be alarming even if there is "normal" arterial flow. - See Ovarian Torsion. Perforated Gastric Ulcer - Review your own films! Radiologists are human too. You know what your concern is and may be able to actively see the important abnormality more easily! - Concerning abdominal exam? You don't need to wait for images to call a surgeon. - Think twice before sending to CT, especially with a concerning abdominal exam. - Resuscitate aggressively! Prepare for the patient to become dramatically more ill! - Don’t forget the broad spectrum antibiotics! Ruptured AAA- Resuscitate! (ABCs, Large Bore Access), but be comfortable with permissive hypotension.
- Target SBP ~80-90 mmHg - Do not be in a hurry to intubate the patient if they are breathing on their own. Many arrest after intubation. - IF you must intubate, VENTILATE SLOWLY. Increased intra-thoracic pressure will crush their already tenuous pre-load and cause an arrest. - Cross-matched PRBCs (consider massive transfusion protocol) - Contact your Vascular Surgeon emergently - At CMC, activate “Code Rupture” Intoxicated with Chest Pain
Infected Kidney Stone
 • Aortoenteric fistula is the abnormal formation of connection between the aorta and bowel, typically occurring the 4th portion of the duodenum.
• Primary fistula formation due to atherosclerotic or infectious erosion of aorta into the bowel; secondary is the result of complications of aortic graft placement, either graft infection or pressure necrosis. • Typically present with “sentinel bleed” followed by massive GI bleed and hemodynamic collapse; classic triad occurs <25% of patients. • Vascular surgery consultation emergently if suspected; CT angiography can be helpful, but only after consultation and surgical evaluation. 
 Thrombotic Thrombocytopenic Purpura:
- Can be hereditary or acquired. Acquired forms can be found as a result of a multitude of disease states. - Patients will more often present with vague symptoms including confusion/AMS rather than focal neurologic deficits attributable to a specific vascular distribution. - Treatment to consider initiating in the ED includes steroids and FFP however be wary of volume in patients with underlying cardiac disease. - VasCath can be placed in ED depending on provider comfort. - Plasma exchange has decreased mortality from 85-95% to 10-20%. Third Degree Heart Block: - Most often seen in elderly patients due to progressive fibrosis and calcification of conduction system and surrounding tissue, but can certainly be a complication of AMI. - Particularly for your elderly patients, be wary of medication side effects. - Atropine is always worth a try. Just realize more often than not it won't help you. - Hypotension? Altered mental status? Distress? PACE THE PATIENT! - Take the time to review initiation of transvenous pacing. Like the infamous ED thoracotomy or cricothyroidotomy, its a procedure we should know like the back of our hands. Final Pearl: if you're going to order an imaging study, look at the WHOLE image. |
Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed
