
0 Comments
Congenital Adrenal Hyperplasia
Always consider adrenal insufficiency in hypotensive patients who remain hypotensive despite appropriate fluid resuscitation and initiation of pressors (whether adult or pediatric)... but particularly think of it in neonates!!
2) Age-based - 0-3 yo: 25mg IV; 3-12 yo: 50mg IV; >12 yo: 100mg IV 3) Randy's Rules (from the brilliant mind of Dr. Cordle) - Give at LEAST 25mg; 3x their current dose; or 2mg/kg 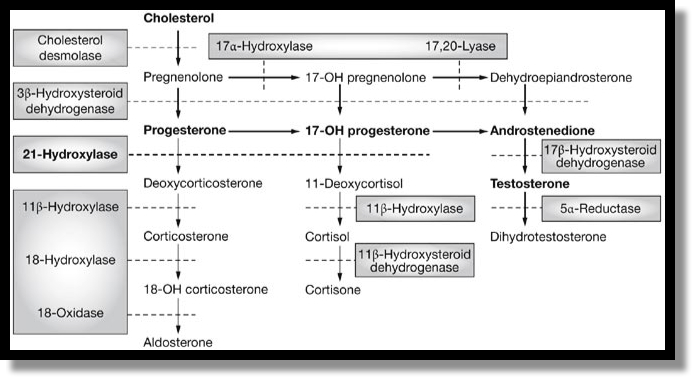 Steroid Production
-- Limitations - requires patient cooperation, not definitive airway. -- Intubate when the above doesn't work - but increased morbidity and mortality with intubation
- Respiratory rate - Short inspiratory time - I:E ratio 1:3 to 1:5 Delayed sequence intubation
10 day old with vomiting
- Hx of "GERD" since day of life 4; Mom GBS + but treated and baby full term without complications; +constipation - Green emesis day of presentation - looks great at bedside - Neonate with Bilious Emesis - KEEP IT SIMPLE... Neonate with Bilious Emesis = Badness until proven otherwise. -- Surgical vs non surgical - Surgical includes duodenal atresia, malrotation with volvulus, NEC. Also consider Sepsis. Malrotation - arrest of normal rotation of embryonic gut > usually presents in infancy -- >50% of kids will present before one month of age -- >90% have vomiting - it won't always be bilious -- > Urgent surgical consultation if kid looks bad - Imaging -- Plain films - not sensitive or sepcific - May see double bubble sign -- Upper GI = study of choice
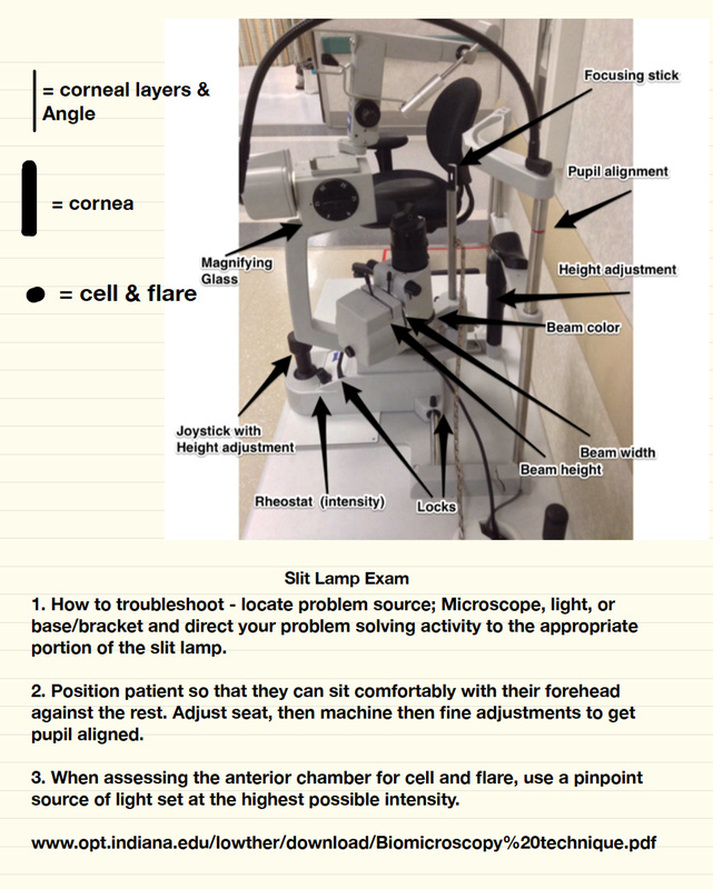
Conjunctivitis: Allergic, viral, bacteria
Uveitis: inflammation of iris, ciliary body, choroid
Acute closed angle glaucoma: emergency need to make dx, can have visual loss.
Myth 4 - The extent of surface burn determines the extent of the injury. Unfortunately, skin findings can be misleading.
Myth 5 - The pathway the electricity takes through the body predicts the pattern of injury. It is helpful to be able to see evidence of the path that the electricity took (ex, from toe to hand), but once again, this can be misleading. Myth 6 - All patients with electric injuries require 24 hours of cardiac monitoring. Most patients who arrive to the ED without having had an arrhythmia and who have a normal ECG with no symptoms do not require prolonged monitoring. Myth 7 - Cardiac monitoring and further testing is always required for TASER injuries. There have been deaths noted with TASER injuries, but these have all been associated with patients who had "excited delirium" -- PCP and TASER is a bad combination. Myth 8 - Victims of lightning injury should not undergo prolonged resuscitation. Lightning victims can have meaningful recoveries after prolonged resuscitation. They can even present with Fixed and Dilated pupils. Do not tell EMS providers to pronounce the victim in the field. Continue to resuscitate and bring them to the ED to further assess.
Back Pain
Indeterminate Ultrasound
High Altitude Cerebral Edema (HACE)
High Altitude Pulmonary Edema (HAPE)
|
Archives
August 2018
Categories
All
|




 RSS Feed
RSS Feed
