 - We are not very good at making the diagnosis…correct as initial diagnosis only 15-50%
- Type A involves ascending aorta and requires immediate cardiothoracic surgeon, Type B does not. - CT Angio is the study of choice in stable patients - Normal CXR in 12% of patients. Abnormal findings include wide mediastinum, abnormal aortic contour, pleural effusion, and wall Ca+ displacement - If no clinically apparent aortic insufficiency or CHF, then treat first with labetalol/esmolol then nitroprusside.
0 Comments
 1. The first key in assessing a patients with dizziness is to define the problem: dizziness is not a medical term, and vertigo is not a diagnosis.
2. If a patient has nystagmus, it is important to interpret and document the nystagmus in a clinically meaningful way which will support your diagnostic decision making. 3. To adequately test the cerebellum, all three of the following must be assessed: limb ataxia, truncal ataxia, and oculomotor control. 4. Correct patient selection is essential when performing the Dix-Hallpike maneuver or the Head Thrust Test. The only patients who are appropriate candidates for the Dix-Hallpike test are those with a history consistent with BPPV. Similarly, the only patients who are appropriate candidates for the head thrust test (and the HINTS exam) are those with acute vestibular syndrome. 5. If the patient has the constellation of signs and symptoms that comprise acute vestibular syndrome, perform the HINTS exam to attempt to distinguish central from peripheral causes 6. Recognize that brain CT rarely identifies early-stage cerebellar infarction. DWMRI is reasonably sensitive for detecting cerebellar infarction early, but it is less sensitive than appropriately performed oculomotor assessment.  Tuberculosis
-Immediately isolate any patient that you believe may have TB, and document that you have done so! -Upper lobe pneumonia should always prompt further consideration of tuberculosis, screen with risk factors -Patients with TB often have multiple ED visits with active disease, risk factors are often overlooked in triage -Remember, PPD and IFN blood testing is for latent TB only and will not help you diagnose active TB -Involve infectious disease, ensure that the health department is involved in the patient's case Elderly Falls - Missed Femoral Neck Fracture -95% due to falls, more than 300k admissions per year -One year mortality in those over 65: 12-37% -High risk of malunion, poor healing, and avascular necrosis if missed -Surgical repair is performed as soon as medically stable for procedure -Range all joints, low threshold to image -Before discharge, consider home/social factors -For a full reassessment, ambulate the patient personally or with the nurse to prevent missed injuries and assess feasibility of discharge High Pressure Injuries -Surgical emergency despite benign exam -Paint/grease guns, pressure washers -Material rapidly spreads to tissue spaces and can cause compartment syndrome -Time Sensitive: Amputation rate 38% within 6 hours, 58% after that -EMS transportation if transferring for ortho evaluation from OSH/Urgent Care 

 Confusion about epinephrine
- Anaphylaxis o Standard: 0.3-0.5 mg IM 1:1,000 (can repeat q5 minutes) o Pediatric: 0.01 mg/kg IM 1:1,000 o Severe/refractory: 0.1mg 1:10,000 IV over 5 minutes + start epinephrine drip - Sources of error include high stress scenarios, confusion about concentrations, multiple concentrations and routes available - Recognize that epinephrine is a medication prone to errors and be clear with orders, double check if need be Rocky Mountain Spotted Fever - Symptoms: Hyponatremia, thrombocytopenia, AMS, fever, abdominal pain/GI symptoms, rash (classically petechial but can vary) - Only about ½ have history of tick exposure - Treat adults and children with doxycycline 100 mg BID in adults, 2.2 mg/kg/dose BID in children. Use chloramphenicol in pregnant females (though less effective than doxycycline). - Doxycyline shortage has resolved, average cost for a 7 day course around $35. Infant Botulism - Presentation: constipation, weakness, intact sensory - Less than 12 months of age (though majority 6wk-6mo) - Diagnose by sending stool sample to CDC - Treatment o More effective if initiated early (within 7 days)– do not wait for confirmation diagnosis o Human derived botulism immunoglobulin (BabyBIG) - $45,000 o Binds free toxin to prevent worsening however will not remove toxin already bound to motor endplate (must sprout new motor endplates for recovery) o Only available through California Department of Health Services – www.infantbotulism.org proves specific instructions on how to acquire immunoglobulin  General 1. WCT algorithms do not work in the real life setting 2. Don’t pay attention to what others have said; you need to evaluate the ECG yourself 3. First question: is the WCT regular or irregular? Sustained Regular WCT I. Differential Diagnosis 1. Sustained regular WCT: most likely ventricular tachycardia (VT) a. Spend 2 minutes searching for P waves – inconsistent P-QRS relationship is 100% specific for VT b. Bizarre QRS morphology that is not c/w RBBB or LBBB (negative QRS in lead I; QRS concordance in the chest leads) strongly supports VT 2. Consider SVT if QRS morphology resembles RBBB or LBBB a. Find an old ECG: are the QRS morphologies identical? b. If no old ECG available, prove SVT by giving IV adenosine c. “I think this is SVT” is not good enough! II. Therapy of Sustained Ventricular Tachycardia 1. Unstable: electric cardioversion 2. Clinically stable: one round of IV antiarrhythmic drug therapy allowed a. IV procainamide may be the most effective agent (avoid in patients with severe systolic CHF and in patients with baseline prolonged QT) b. IV amiodarone c. Consider IV propranolol or IV metoprolol in ischemic VT and in patients with “electric storm” (repeat episodes of VT/VF) Sustained Irregular WCT I. Differential Diagnosis 1. Sustained irregular WCT: most likely not VT but atrial fibrillation (AF) 2. Rate 120-160; QRS morphology is c/w RBBB or LBBB: AF with bundle branch block 3. Rate very fast; QRS morphology is bizarre, not c/w RBBB or LBBB: most likely AF with WPW (FBI – Fast, Broad-complex, Irregular) II. Therapy 1. AF with BBB: usual therapy for AF (IV diltiazem etc.) 2. AF with WPW (“FBI”) a. Clinically unstable or ventricular rate excessive: electric cardioversion b. Clinically stable: IV procainamide or IV ibutilide c. Clinically very stable, rate not very fast: PO flecainide or propafenone NOT ALLOWED: IV verapamil, diltiazem, digoxin, adenosine 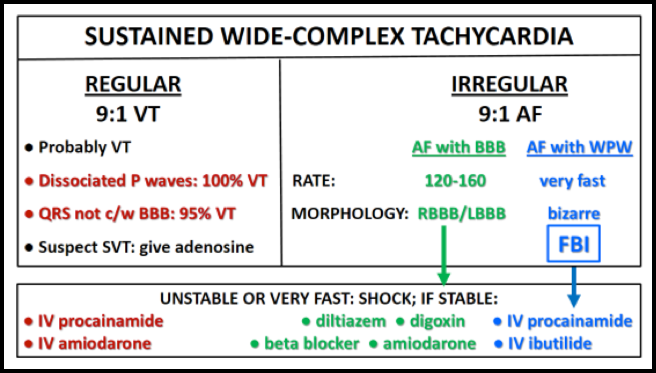  · Erections lasting more than 4 hours are a medical emergency.
· Secondary to impaired contraction of corporal smooth muscle. · Immediate aspiration/irrigation and/or injection of phenylephrine are the mainstay of treatment. · Don’t be afraid to use a big needle.  Myocarditis:
- broad spectrum of disease, high level of suspicion is essential - myocarditis can mimic STEMI and Wellens syndrome among others - EKG, echo, and cardiac enzymes cannot rule in/out the diagnosis - No hesitation to consult Peds Cards NAT: - no discrimination, occurs in all people groups - history, exam, and physical findings may raise suspicion for abuse. - must place child in gown. - make sure story matches up... loose ends must be tied Marfan and PTX: - Must be personally knowledgeable about equipment associated with procedures (ie: suction device for chest tubes) - Pigtail catheters equivalent to thoracostomy tubes for uncomplicated PTX with decreased pain - http://pedemmorsels.com/pigtail-catheter/ |
Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed
