|
Case 1 - Post-Operative Pneumoperitoneum and Perforated Marginal Ulcer After Roux-en-Y
Case 2 - Complications of Chronic Suppurative Otitis Media (CSOM)
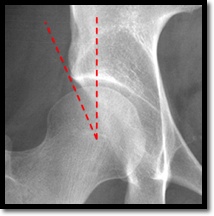
Important Radiographic Signs to Identify on AP Pelvis/Hip
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
Archives
August 2018
Categories
All
|

 RSS Feed
RSS Feed
