|
1. Signs and symptoms of an Upper GI bleed in the pediatric patient
-most common presentation is hematemesis -melena also common presentation -many things mimic GI bleed -> food coloring, raw meats, swallowed blood from oropharynx 2. Differential diagnosis for acute pediatric upper GI bleed -determine if variceal vs nonvariceal -variceal bleed (uncommon but can be life threatening)-> portal HTN from congenital liver pathologies -mucosal bleed -> gastritis, esophagitis, caustic ingestion, foreign body most common in pediatrics 3. ED diagnostic workup for an upper GI bleed in a pediatric patient -CBC, BMP, LFT's, and Type/Cross essential to the workup 4. ED Management of Pediatric Upper GI bleed patient -Place an NG tube -Get GI, Surgery, and Interventional Radiology Involved early -Octreotide and vasopressin are important treatments for variceal bleed -For mucosal bleeds control acid production
0 Comments
 - Neonate in respiratory distress: remember NRP! - Neonate in respiratory distress with true unilateral absent breath sounds = Congenital Diaphragmatic Hernia??!!-> confirm with CXR Congenital Diaphragmatic Hernia (CDH) - Neonates likely have high risk for pulmonary hypertension! - Do not give PPV -> worsens GI distention/lung compression = worsening pulmonary HTN - In neonates intubate early to prevent hypoxia (hypoxia worsens pulmonary HTN) with low pressure vent settings - Maintain systemic BP to reduce right to left shunting - Older children with CDH, less likely to have significant pulmonary HTN, keep calm and try to avoid intubation - Persistent/worsening cyanotic neonate - think cyanotic congenital heart defect -> Start Prostaglandins - Remember Prostaglandins cause apnea, will likely need intubation - Neonate in extremis = call for back-up early! 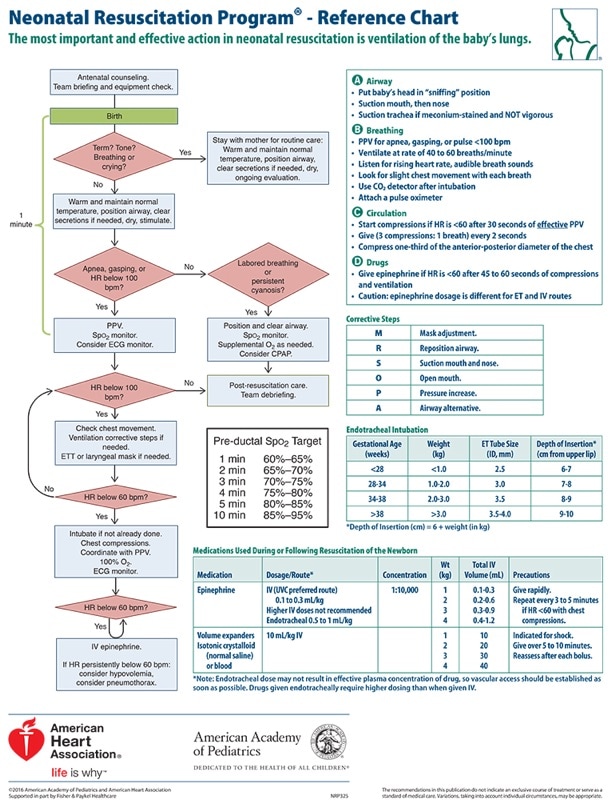 
- severe onset of symptoms - worsening clinical course
 Abdominal Pain of Unusual Cause
PE vs Sepsis


 • The pediatric airway has known unique challenges. Prepare yourself physically and cognitively!
• Maintain spontaneous ventilation if there is any doubt about obtaining successful advanced airway. • Practice using airway equipment when you don't need it, so you are ready when you do need it.  Septic arthritis of the hip
-Most common hematongenous spread - Up to 20% of patients with non-gonococcal septic arthritis will have 2 or more joints involved –> always do a full musculoskeletal exam! - 50% will have positive blood cultures –> always obtain cultures. - Risk factors: Extremes of age, hardware/recent instrumentation, skin infection, underlying arthritis, IV drug use - You cannot rule out septic arthritis with inflammatory markers or any physical exam findings, so err on the side of obtaining joint fluid. Pediatric septic arthritis vs. transient synovitis - Kocher criteria can help differentiate: Temperature >38.5, WBC >12K, ESR >40, unable to bear weight.
Contrast Extravasation
Spontaneous Pneumomediastnum
 Define status epilepticus:
Consider etiologies:
Remember ABCs and supportive care in addition to treating seizures Learn dosing for hypoglycemic seizure with dextrose
Learn dosing for hyponatremia seizure with 3% NaCl Medications First line:
Second line:
Refractory/Third line:
|
Archives
August 2018
Categories
All
|
 RSS Feed
RSS Feed
