|
HPI: 90 yo male with PMH of HTN, DM presents to ED with 2-3 weeks of lower extremity edema and intermittent chest pain, with acute worsening of cardiac chest pain yesterday and this morning, now accompanied by SOB, nausea, and lightheadedness. Evaluated in major and found to have a heart rate 40s-60s. ECG: 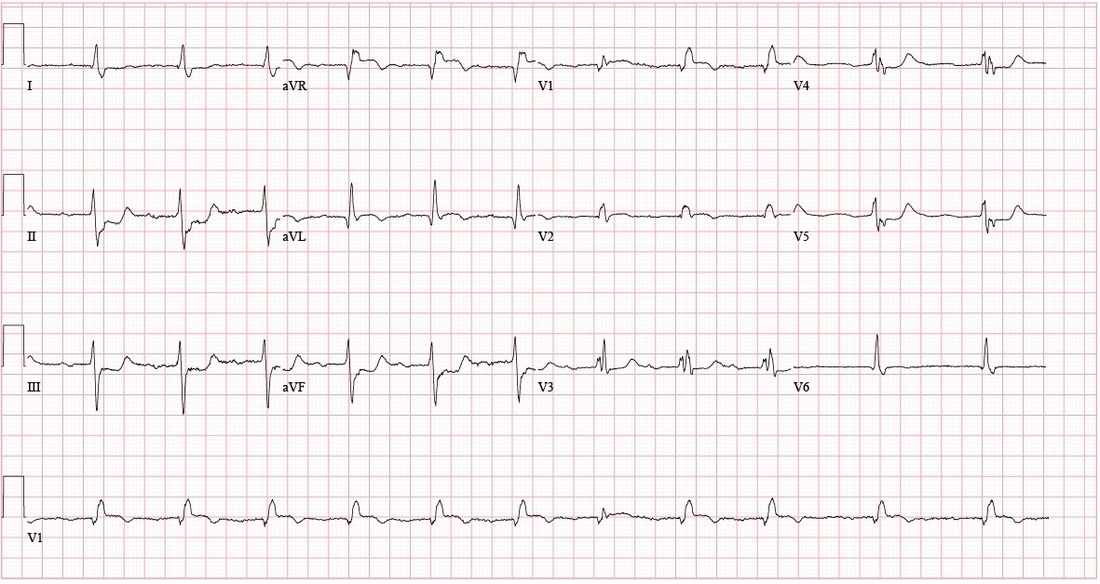 Questions: How is a bifascicular block diagnosed? What are the clinical implications of the bifascicular block? What about in the context of a first degree AV block? ECG Interpretation: Sinus rhythm, rate 69, with sinus arrhythmia and First Degree AV Block. PR interval 272. QRS 150. QTc 490. Left Axis Deviation. (QRS is upward in I and downward in II) Right BBB + Left Anterior Fascicular Block = Bifascicular Block Subtle ST Elevation V1 and V2; consider anterolateral STEMI ST depression inferior leads; inferior ischemia vs. reciprocal changes from anterolateral STEMI Discussion: 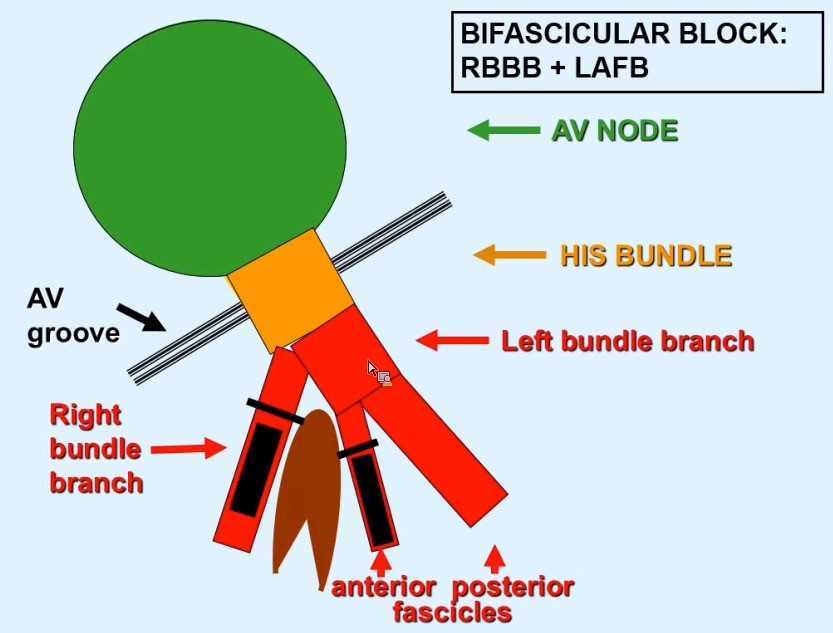 Definitions: (LAFB = Left Anterior Fasicular Block; RAFB = Right Anterior Fascicular Block )
• Bifascicular block: RBBB + either LAFB or RAFB o RBBB + Left Axis Deviation (<-45) = LAFB o RBBB + Right Axis Deviation (>+90)= RAFB • Incomplete Trifascicular block: Conduction damage to all three fascicles o Bifascicular block + first degree AV block OR o Bifascicular block + second degree AV Block OR o RBBB+ Alternating LAFB/LPFB Implications: o In an asymptomatic patient, bifascicular block is largely incidental and no workup is indicated. o If the patient presents with syncope and bifascicular block, this is a medical emergency and the American College of Cardiology and AHA recommend pacemaker implantation. o Risk of progression to complete heart block thought to be low (1% per year in a cohort of 554 patients), but some studies have suggested rates as high as 16% in RBBB + LAFB and 21-75% in RBBB + RAFB. Higher risk in a retrospective review prior to modern reperfusion therapy. o Patients with incomplete trifascicular block are thought to have a greater risk of progression to complete heart block, though data are not conclusive Patient course: Admitted to ICU with systolic pressure in 70s, felt to be cardiogenic shock secondary to MI. Patient was treated with 1 amp of atropine, which improved heart rate from 40s to 70s. Initial troponin was 3.41, which plateaued at 84 on 9/8. No ST elevation. Poor cath candidate given age, AKI at presentation. Treated medically (ASA, statin, Plavix, heparin gtt, carvedilol) and has been transferred to the floor, now hemodynamically stable. Last ECG relatively unchanged since admission (persistent first degree AV block, RBBB, LAFB, ST depression. References: • Dr. Littmann’s ECG Lectures (graphic also from Dr. Littmann) • http://lifeinthefastlane.com/ecg-library/basics/bifascicular-block/ • Uptodate sections on “Conduction Abnormalities after Myocardial Infarction” and “Course and Treatment of Bifascicular Block” • ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Circulation. 2008;117(21):e350. By: Dean Tanner, PGY1
0 Comments
HPI: 50-year-old man with PMH of HTN, DM, ESRD on dialysis, and polysubstance abuse with a one-year history of recurrent chest pain and multiple visits to the emergency department for chest pain exacerbations. He was recently seen for left-sided chest pain with an EKG showing nonspecific ST depressions, negative chest x-ray, and elevated troponins ×3, peaked at 1.31. He did not undergo cardiac catheterization due to recent cocaine use. He returns today with 10/10 chest pain refractory to nitro taken at home. ECG: 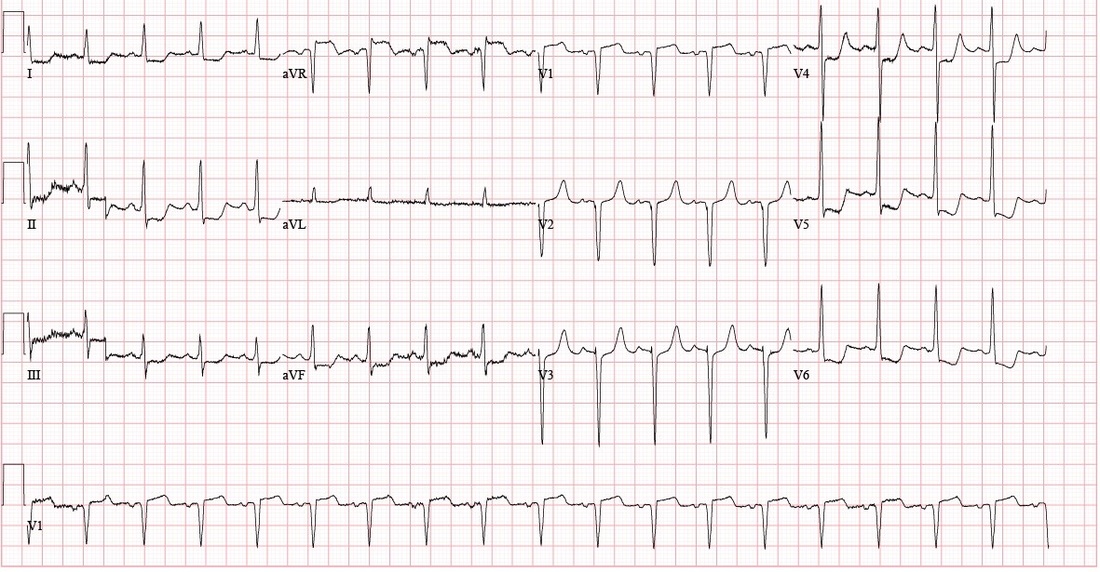 ECG Interpretation: Sinus tachycardia with rate of 108. PR and QRS intervals normal. Probable LVH. Anterior Q waves, possibly due to LVH. ST depression inferiorly and laterally. ST elevation 2 mm in aVR and 1 mm in V1. Patient course: Underwent successful emergent cardiac catheterization. LAD 90-95% occlusion, LAD-1st Diagonal 90% occlusion, LMCA 50% occlusion, proximal RCA 90% occlusion (stented later). Peak troponin 26.70. 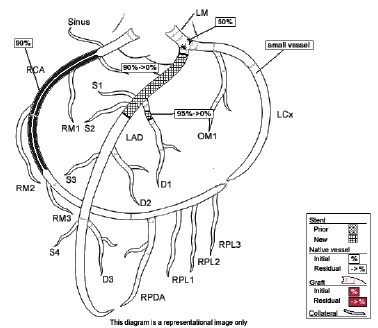 Discussion: aVR sign: possible Left Main Coronary Artery (LMCA) occlusion or other severe coronary disease (proximal LMA, 3-vessel disease) • When associated with angina and diffuse ST-segment depression o ST elevation in aVR ≥ 1mm is 80% specific for severe LMCA disease or 3-vessel disease. (LAD + LAD-D1 in this case) o ST elevation in aVR > V1 typically signifies LMCA over proximal LAD  o If STE in aVR is not > V1, more likely proximal LAD occlusion
o STE in aVR is associated with very high mortality. STE > 1mm associated with 6-7 fold increase in mortality STE > 1.5mm associated with 20-75% mortality • When associated with STE of other leads, aVR STE is independently associated with increased mortality. Pro Tips: • Patients with ≥ 1 mm STE in aVR may potentially require early/urgent CABG; discuss with cardiology or CT surgery prior to giving Clopidogrel/Prasugrel (thienopyridines 7 or less days before CABG is associated with increase in major bleeding). • Presence of aVR sign may not meet criteria for a Code STEMI, but it should be recognized as a STEMI equivalent and and requires urgent reperfusion therapy References: • http://lifeinthefastlane.com/ecg-library/lmca/ • Kosuge M, Ebina T, Hibi K, Morita S, Endo M, Maejima N, Iwahashi N, Okada K, Ishikawa T, Umemura S, et al. An early and simple predictor of severe left main and/or three-vessel disease in patients with non-ST-segment elevation acute coronary syndrome. Am J Cardiol. 2011;107:495–500 • Tamura, A. Significance of lead aVR in acute coronary syndrome. World Journal of Cardiology, 2014; 6(7): 630-637. • Dr. Littmann’s ECG video lectures HPI: 50-year-old African-American female with PMH of untreated hypertension, CKD secondary to membranous glomerulonephritis, possible schizophrenia, ongoing cocaine abuse (last use 3 days prior to admission), admitted for treatment of CAP. Chest CT showed bilateral lower lobe infiltrates with moderate pericardial effusion and small bilateral pleural effusions. Cardiology consulted for concern for pericardial tamponade, as primary team reported continued shortness of breath and findings of pulsus paradoxsus and electrical alternans on EKG. EKG: 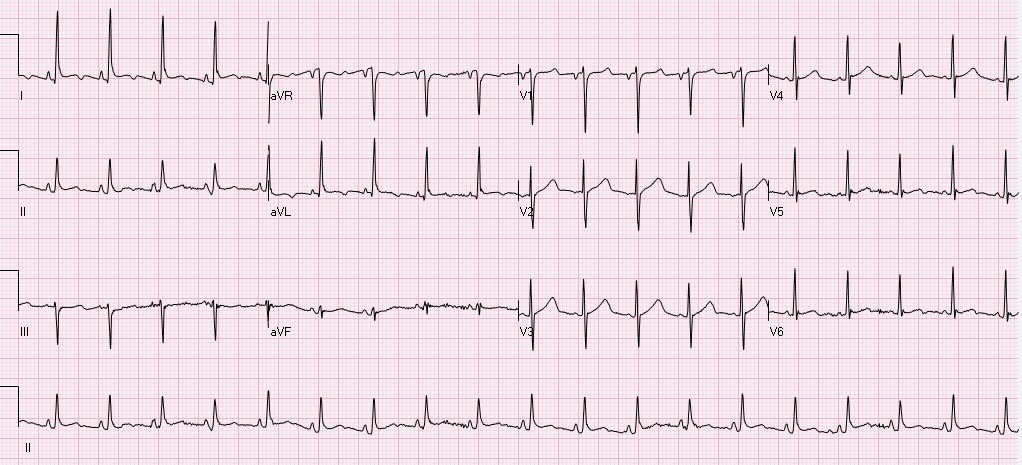 Questions: What does cardiac tamponade look like on an EKG? Does this EKG exhibit electrical alternans and confirm the presence of cardiac tamponade? How sensitive/specific is EKG in detecting cardiac tamponade? EKG Interpretation: Sinus tachycardia with a rate of 114. Horizontal axis. Normal voltage. Borderline LVH. Nonspecific T wave abnormalities, no significant ST depression or elevation. Artifact consistent with respiratory variation. Discussion: EKG findings and Sensitivity/Specificity for cardiac tamponade: • Sinus tachycardia o Sensitivity 76%, Specificity 60% 1 o OR: 4.9 (95% CI: 2.22-10.80) • Low QRS voltage o Sensitivity 56%, Specificity 74% 1 o OR: 3.7 (95% confidence interval [CI]: 1.65-8.30) • Electrical alternans o Sensitivity 23%, Specificity 98% 1 o OR: 12.3 (95% CI: 1.58-95.17) o Electrical alternans is characterized by a cyclical, beat-to-beat shift in the QRS axis, caused by the heart swinging back and forth like a pendulum in a large pericardial effusion relative to the stationary EKG leads. 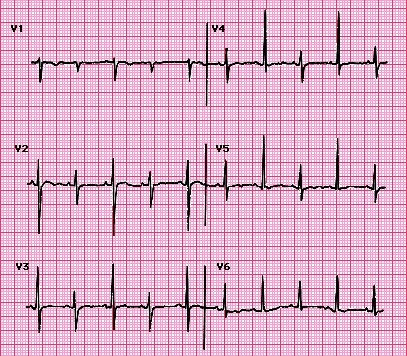 o Video: http://www.nejm.org/doi/full/10.1056/NEJMicm1408805 o This is in comparison to this patient’s EKG, which shows normal respiratory variation over several beats, more notably in her V1 rhythm strip below. These are more pronounced in this patient as she was dyspneic and tachypneic given her pulmonary disease. o Normal respiratory variation:  • Presence of all 3 (Sensitivity 8%, Specificity 100%) 1
Does our patient have cardiac tamponade? • EKG does reveal sinus tachycardia, but not electrical alternans or low voltage. We relied on echocardiogram and clinical presentation to confirm that the patient did not, in fact, have cardiac tamponade. Pro-tip: • Do not rely on EKG alone for diagnosis of or screening for cardiac tamponade. • Do not confuse respiratory variation with electrical alternans on EKG. By: Dean Tanner, PGY1 Resources: 1. Role of a 12-lead electrocardiogram in the diagnosis of cardiac tamponade as diagnosed by transthoracic echocardiography in patients with malignant pericardial effusion. Argula, RG, et al. Clin Cardiol. 2015 Mar;38(3):139-44. doi: 10.1002/clc.22370. Epub 2015 Feb 18. 2. Electrical Alternans with Pericardial Tamponade. Jehangir, W, Osman, M. N Engl J Med 2015; 373:e10August 20, 2015DOI: 10.1056/NEJMicm1408805 |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
