|
HPI: 20 y/o otherwise healthy male presents after syncopal event while playing basketball. He is athletic, plays basketball 7 days a week, and has never syncopized before. There was a prodromal sensation of “lightheadedness”, but he denies other symptoms and is asymptomatic upon ED arrival. EKG is obtained immediately: EKG: 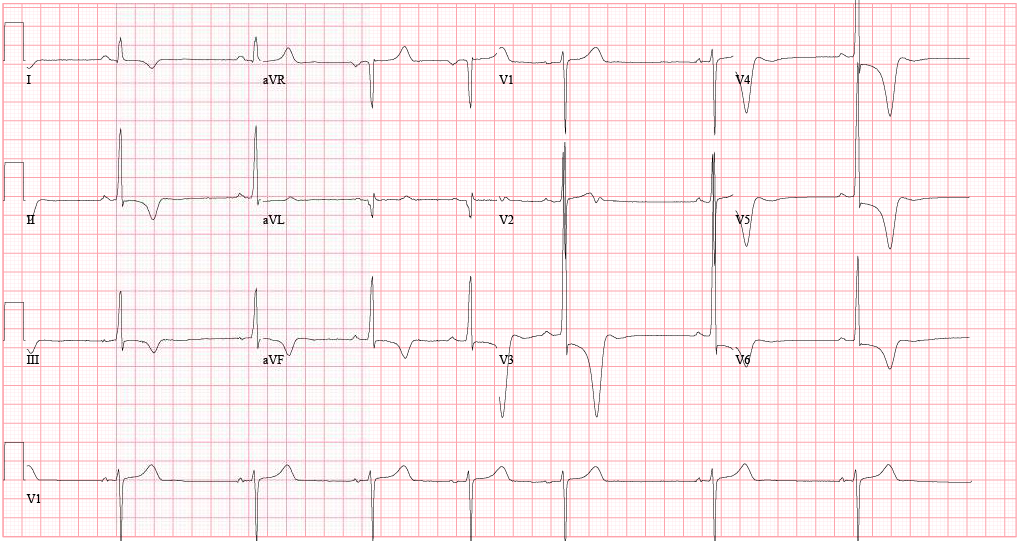 EKG Interpretation:
Sinus bradycardia (46 bpm) w/ profound LVH and repolarization abnormality, diffuse ST depression and T-wave inversions. No prior EKG to compare. Discussion: Large negative T-waves have a broad DDx, including ACS, cocaine toxicity, CNS disorders, metabolic abnormalities, etc. In addition, LVH is a common incidental finding on EKG as well. In a young healthy patient without HTN or aortic stenosis, LVH should raise clinical suspicion for Hypertrophic Cardiomyopathy (HC). Additionally, large deep symmetrical T-wave inversions are typical for the Apical Variant of HC (only 3-5% of total HC cases). Importantly, since there is no LV outflow tract obstruction in this variant, the classic murmur associated with Hypertrophic Obstructive Cardiomyopathy (HOCM) will be absent. Bedside echocardiography confirms the diagnosis. Why is this important? Approximately 1/3 of patients may go on to develop life-threatening complications if untreated. In particular, ventricular arrhythmias. Close monitoring/follow-up is needed, and permanent ICD should be considered. Management: • Continuous cardiac monitoring, ACS evaluation w/ serial troponin and EKGs • Immediate bedside echocardiography • Cardiology consultation and ultimately ICD placement • Longterm avoidance of competitive sports or other intense physical activities By Dr. Blake Johnson References: 1. Siewe D, Nichols K, Furney S, Littmann L. King of Hearts for Ace of Spades: Apical Hypertrophic Cardiomyopathy. Am J of Med. 2014; vol 127 (1): 31-33. 2. Eriksson MJ, Sonnenberg B, Woo A, et al. Long-term outcome in patients with apical hypertrophic cardiomyopathy. J Am Coll Cardiol. 2002;39(4):638-645.
0 Comments
HPI: 55 y/o male with no past medical history presents with vague symptoms including nausea, lethargy, and weakness. Vital signs are within normal limits. Before labs come back you obtain this EKG: EKG: 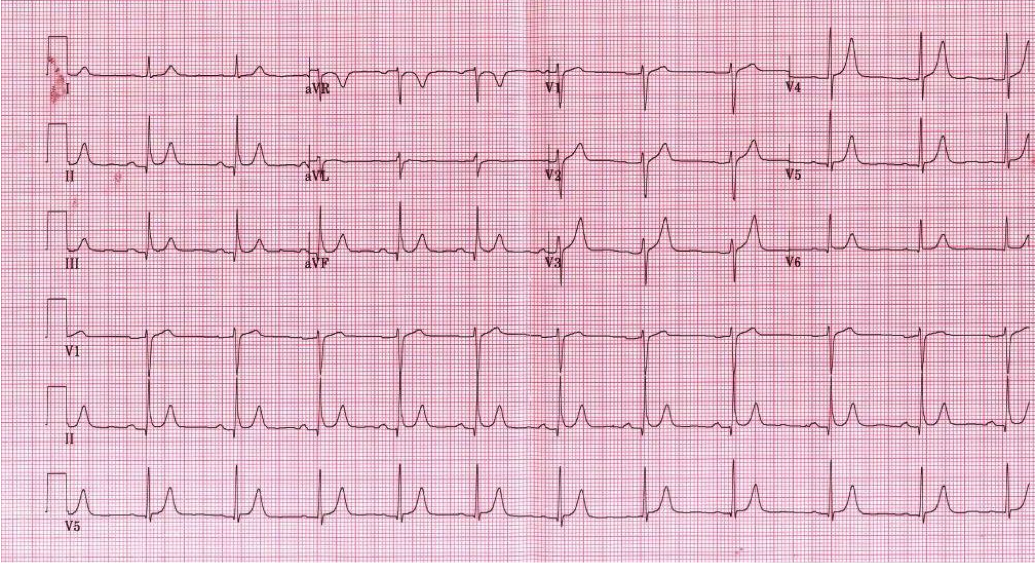 EKG Interpretation: Normal sinus rhythm, rate 67 bpm. Normal axis. Narrow QRS, no ST elevation or depression. --> “Normal ECG”. **On closer inspection you notice the QT interval appears shortened, calculated at 350 ms** Discussion: Initial labs show total calcium of 15.0 mg/dL and PTH of 400 pg/mL (nl 7-53 pg/mL). A single large parathyroid adenoma was diagnosed and subsequently removed. EKG signs of Hypercalcemia: · Short QT interval, usually less than 350 ms · In severe hypercalcemia, can see Osborn waves (J waves) · In extreme hypercalcemia, ventricular irritability and ventricular fibrillation have been reported Remember, degree of EKG findings usually signify severity of hypercalcemia! Administer fluid resuscitation and treat the underlying cause. Simplified DDx for shortened QT interval: 1) Hypercalcemia 2) Congenital short QT syndrome 3) Digitalis toxicity 4) Normal variant. 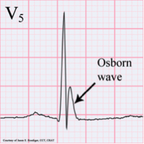 By Dr. Blake Johnson
HPI: Approximately 30 year old female with history of frequent PVCs presents via EMS with palpitations and near syncope. She was driving on the highway today when she had to stop due to abrupt palpitations, SOB, and sensation like she was about to “black out”. EKG: 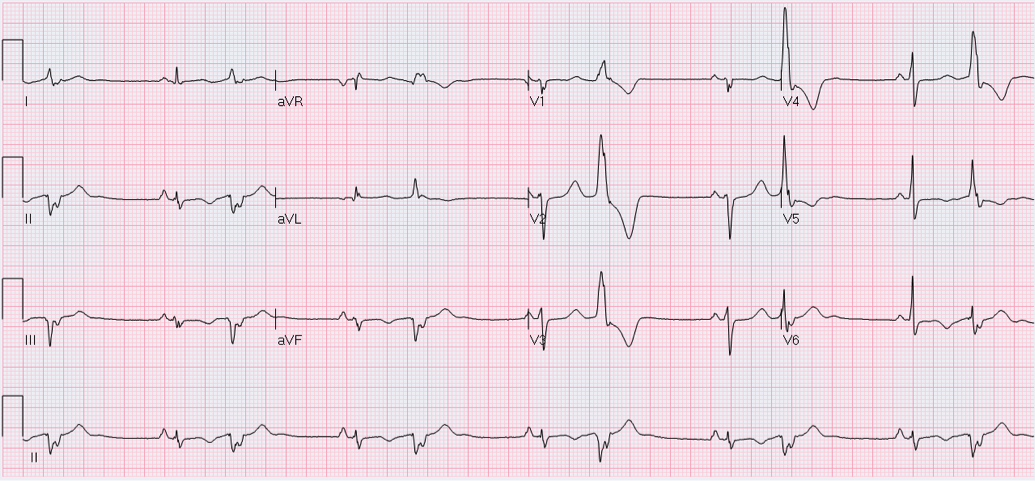 EKG Interpretation:
Sinus rhythm with monomorphic PVCs in pattern of bigeminy. Horizontal axis. Inverted T-waves in inferolateral leads (II, III, aVF, V5-V6). Machine says to consider INFEROLATERAL ISCHEMIA. Discussion: Is this ischemia? No. Patient is young and otherwise healthy with no risk factors for cardiovascular disease. She has a history of frequent ventricular ectopy, and presentation is concerning for transient ventricular tachycardia. Pattern of T-wave inversions is consistent with “Cardiac Memory”. How to differentiate: · Clinical scenario not consistent with ACS · Negative T-waves in same leads where PVCs are negative · Eventual resolution after resumption of normal electrical activation Extent and duration of effect correlates with duration of preceding abnormal ventricular conduction. The longer and more profound the electrical disturbance, the longer and more profound Cardiac Memory persists. Most commonly seen with: 1) Ventricular pacing 2) Intermittent LBBB 3) Pre-excitation in WPW 4) Episodes of ventricular ventricular tachycardia (likely cause in our patient). Management: · High index of suspicion for underlying pathology · Provider awareness of phenomenon so as not to initiate unnecessary interventions (Cath lab, etc.) · Treatment aimed at underlying derangement as appropriate · Inpatient vs. outpatient continuous cardiac monitoring if diagnosis in question By Dr. Blake Johnson HPI: Patient is a 54-year-old male presenting with palpitations and near syncope. Patient states that he was told he had a “heart problem” as a child. He was diagnosed with atrial fibrillation some 10+ years ago. EKG: 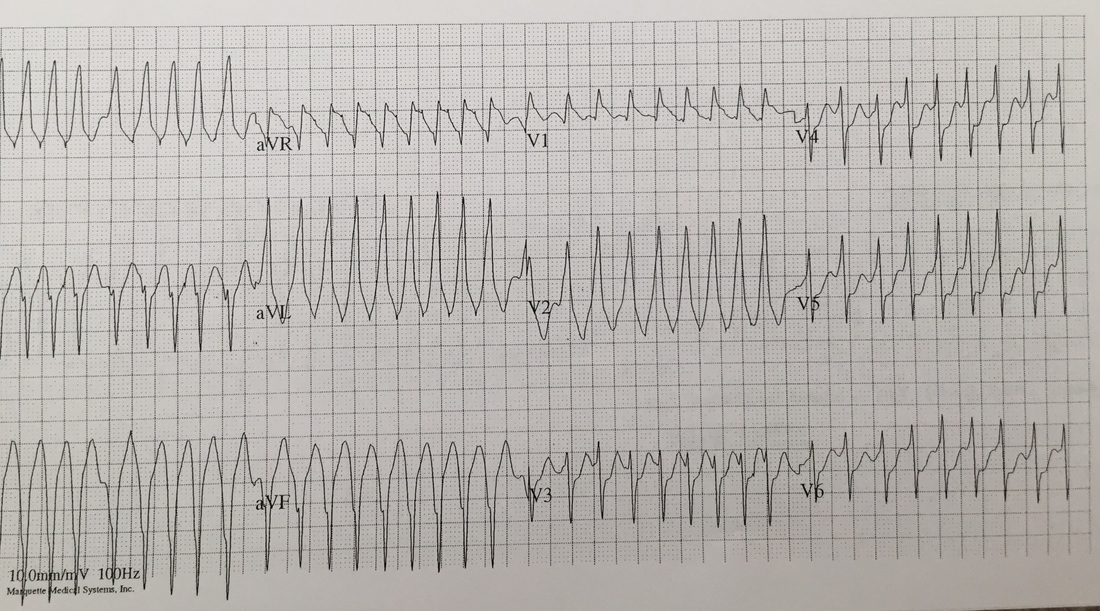 EKG Interperitation:
Rate estimated to be in the high 100s and irregularly irregular. QRS is wide. There are no appreciable P waves. Does not fit any typical bundle branch pattern. Discussion: Is this V tach? No. The patient has a wide complex irregulary irregular waveform. This is MOST likely to be a patient with WPW and a-fib. This is easily confused with ventricular tachycardia. How to differentiate: · Irregularly irregular · Rapid · Wide complex · Does not fit bundle branch pattern · No P waves Treatment: · DO NOT give: adenosine, verapamil, diltiazem, digoxin, beta blocker or amio o Due to the presence of accessory pathway blocking down the AV node, may cause the accessory pathway to become the primary driver of conduction. · Treated with IV procainamide if clinically stable. Dose is 15-16 mg/kg given at a rate no faster than 50 mg/min. · If unstable: Immediate DC cardoversion · Patients will require admission with likely EP study. By Dr Andrew Puchiaty |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
