|
HPI: 50-year-old man with PMH of HTN, DM, ESRD on dialysis, and polysubstance abuse with a one-year history of recurrent chest pain and multiple visits to the emergency department for chest pain exacerbations. He was recently seen for left-sided chest pain with an EKG showing nonspecific ST depressions, negative chest x-ray, and elevated troponins ×3, peaked at 1.31. He did not undergo cardiac catheterization due to recent cocaine use. He returns today with 10/10 chest pain refractory to nitro taken at home. ECG: 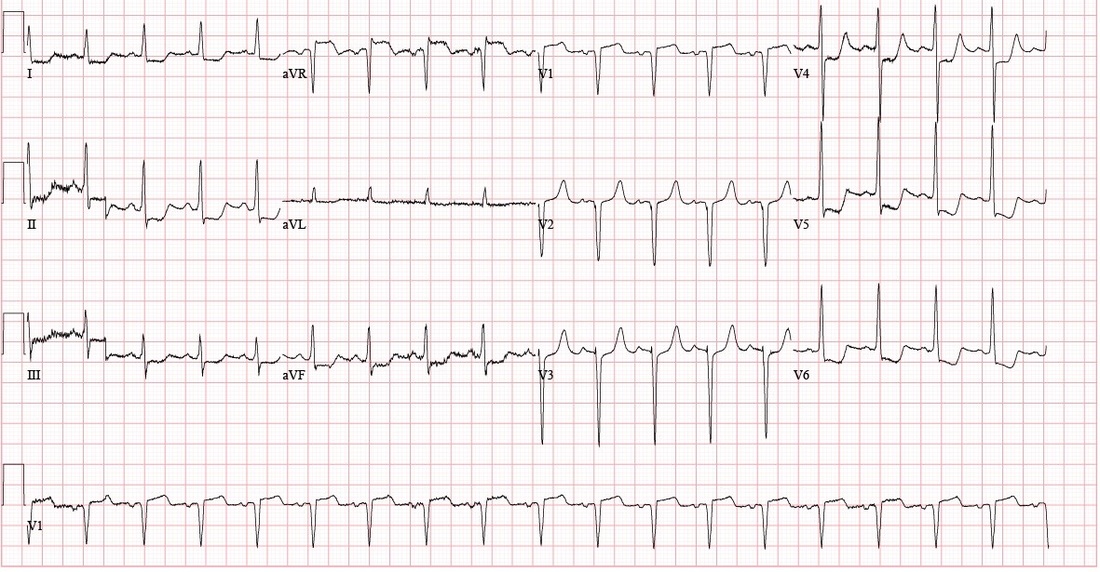 ECG Interpretation: Sinus tachycardia with rate of 108. PR and QRS intervals normal. Probable LVH. Anterior Q waves, possibly due to LVH. ST depression inferiorly and laterally. ST elevation 2 mm in aVR and 1 mm in V1. Patient course: Underwent successful emergent cardiac catheterization. LAD 90-95% occlusion, LAD-1st Diagonal 90% occlusion, LMCA 50% occlusion, proximal RCA 90% occlusion (stented later). Peak troponin 26.70. 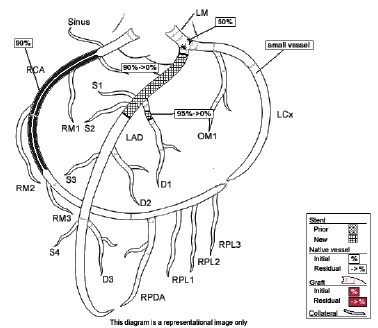 Discussion: aVR sign: possible Left Main Coronary Artery (LMCA) occlusion or other severe coronary disease (proximal LMA, 3-vessel disease) • When associated with angina and diffuse ST-segment depression o ST elevation in aVR ≥ 1mm is 80% specific for severe LMCA disease or 3-vessel disease. (LAD + LAD-D1 in this case) o ST elevation in aVR > V1 typically signifies LMCA over proximal LAD  o If STE in aVR is not > V1, more likely proximal LAD occlusion
o STE in aVR is associated with very high mortality. STE > 1mm associated with 6-7 fold increase in mortality STE > 1.5mm associated with 20-75% mortality • When associated with STE of other leads, aVR STE is independently associated with increased mortality. Pro Tips: • Patients with ≥ 1 mm STE in aVR may potentially require early/urgent CABG; discuss with cardiology or CT surgery prior to giving Clopidogrel/Prasugrel (thienopyridines 7 or less days before CABG is associated with increase in major bleeding). • Presence of aVR sign may not meet criteria for a Code STEMI, but it should be recognized as a STEMI equivalent and and requires urgent reperfusion therapy References: • http://lifeinthefastlane.com/ecg-library/lmca/ • Kosuge M, Ebina T, Hibi K, Morita S, Endo M, Maejima N, Iwahashi N, Okada K, Ishikawa T, Umemura S, et al. An early and simple predictor of severe left main and/or three-vessel disease in patients with non-ST-segment elevation acute coronary syndrome. Am J Cardiol. 2011;107:495–500 • Tamura, A. Significance of lead aVR in acute coronary syndrome. World Journal of Cardiology, 2014; 6(7): 630-637. • Dr. Littmann’s ECG video lectures
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
