|
HPI: 50-year-old African-American female with PMH of untreated hypertension, CKD secondary to membranous glomerulonephritis, possible schizophrenia, ongoing cocaine abuse (last use 3 days prior to admission), admitted for treatment of CAP. Chest CT showed bilateral lower lobe infiltrates with moderate pericardial effusion and small bilateral pleural effusions. Cardiology consulted for concern for pericardial tamponade, as primary team reported continued shortness of breath and findings of pulsus paradoxsus and electrical alternans on EKG. EKG: 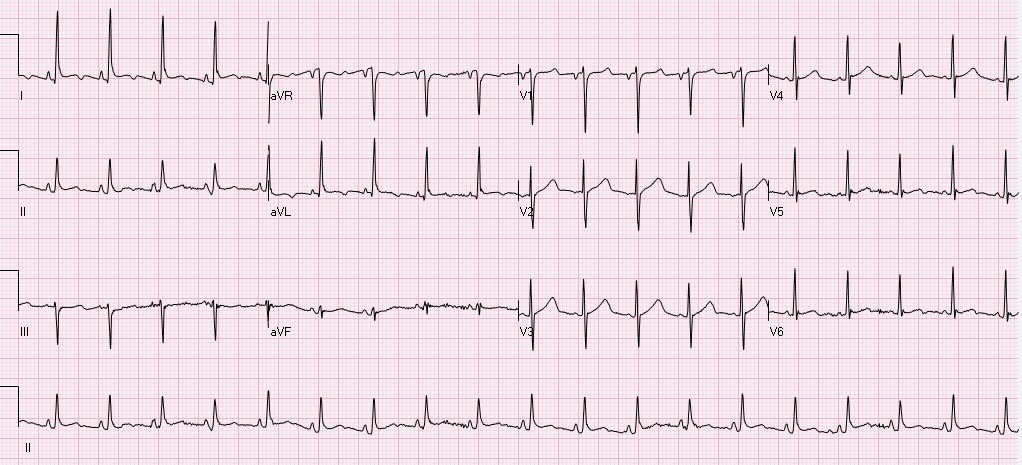 Questions: What does cardiac tamponade look like on an EKG? Does this EKG exhibit electrical alternans and confirm the presence of cardiac tamponade? How sensitive/specific is EKG in detecting cardiac tamponade? EKG Interpretation: Sinus tachycardia with a rate of 114. Horizontal axis. Normal voltage. Borderline LVH. Nonspecific T wave abnormalities, no significant ST depression or elevation. Artifact consistent with respiratory variation. Discussion: EKG findings and Sensitivity/Specificity for cardiac tamponade: • Sinus tachycardia o Sensitivity 76%, Specificity 60% 1 o OR: 4.9 (95% CI: 2.22-10.80) • Low QRS voltage o Sensitivity 56%, Specificity 74% 1 o OR: 3.7 (95% confidence interval [CI]: 1.65-8.30) • Electrical alternans o Sensitivity 23%, Specificity 98% 1 o OR: 12.3 (95% CI: 1.58-95.17) o Electrical alternans is characterized by a cyclical, beat-to-beat shift in the QRS axis, caused by the heart swinging back and forth like a pendulum in a large pericardial effusion relative to the stationary EKG leads. 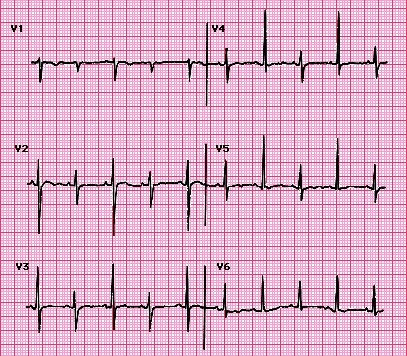 o Video: http://www.nejm.org/doi/full/10.1056/NEJMicm1408805 o This is in comparison to this patient’s EKG, which shows normal respiratory variation over several beats, more notably in her V1 rhythm strip below. These are more pronounced in this patient as she was dyspneic and tachypneic given her pulmonary disease. o Normal respiratory variation:  • Presence of all 3 (Sensitivity 8%, Specificity 100%) 1
Does our patient have cardiac tamponade? • EKG does reveal sinus tachycardia, but not electrical alternans or low voltage. We relied on echocardiogram and clinical presentation to confirm that the patient did not, in fact, have cardiac tamponade. Pro-tip: • Do not rely on EKG alone for diagnosis of or screening for cardiac tamponade. • Do not confuse respiratory variation with electrical alternans on EKG. By: Dean Tanner, PGY1 Resources: 1. Role of a 12-lead electrocardiogram in the diagnosis of cardiac tamponade as diagnosed by transthoracic echocardiography in patients with malignant pericardial effusion. Argula, RG, et al. Clin Cardiol. 2015 Mar;38(3):139-44. doi: 10.1002/clc.22370. Epub 2015 Feb 18. 2. Electrical Alternans with Pericardial Tamponade. Jehangir, W, Osman, M. N Engl J Med 2015; 373:e10August 20, 2015DOI: 10.1056/NEJMicm1408805
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
