|
HPI: Approximately 30 year old obese gentleman with 15 pack year smoking history presents with 2 days SOB, cough productive of yellow sputum, and occasional chest pain. He has a family history significant for MI at a young age so an EKG is obtained. EKG: 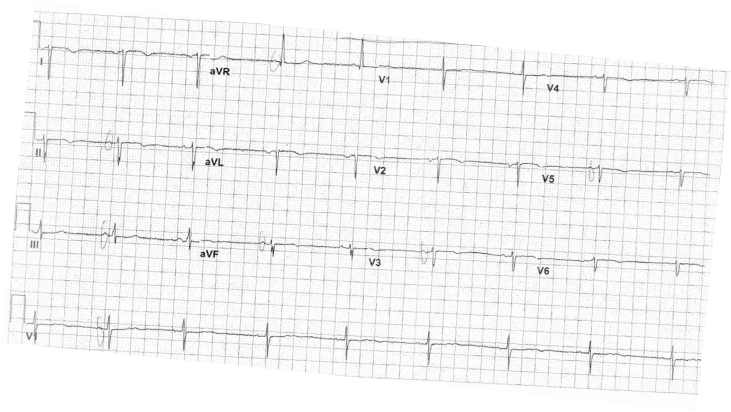 EKG Interpretation:
Heart rate is <60 and regular. This EKG is not in sinus rhythm. P waves are inverted in I and upright in avR. There is significant axis deviation with QRS down going in lead I and II. QRS normal width. Abnormal R wave progression with QRS upgoing in lead V1 and R wave highest in V1. No ST changes. QT interval within normal. Inverted T waves in V2-V5. Discussion: Differential for inverted P waves in lead 1 should always include the following:
In dextrocardia the QRS is down going in lead I and the R wave progression is the opposite. R wave is highest in V1. The net vector is no longer going towards the left leg. This patient has dextrocardia Management: How do you confirm this? 1. Reverse all the leads, chest and limb leads and repeat the EKG. This will allow you to properly interpret any abnormalities on the EKG. 2. Obtain a chest x-ray to confirm dextrocardia 3. Inform patient of the diagnosis and if possible give patient a copy of his EKG or make a note in the patient chart. 4. If defibrillating a patient with dextrocardia, remember to place the pads in reverse position. Dextrocardia Pearls: There are two main types of dextrocardia: dextrocardia of embryonic arrest and dextrocardia situs inversus. In dextrocardia embryonic arrest, the heart is simply found more right in the chest cavity than normal. In dextrocardia situs inversus, the heart is a mirror image situated on the right. If all visceral organs are inverted, it is called dextrocardia situs inversus totalis. Dextrocardia has a prevalence of approximately 1 in 12,000 people.
0 Comments
|
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
