|
HPI: 90 yo male with PMH of HTN, DM presents to ED with 2-3 weeks of lower extremity edema and intermittent chest pain, with acute worsening of cardiac chest pain yesterday and this morning, now accompanied by SOB, nausea, and lightheadedness. Evaluated in major and found to have a heart rate 40s-60s. ECG: 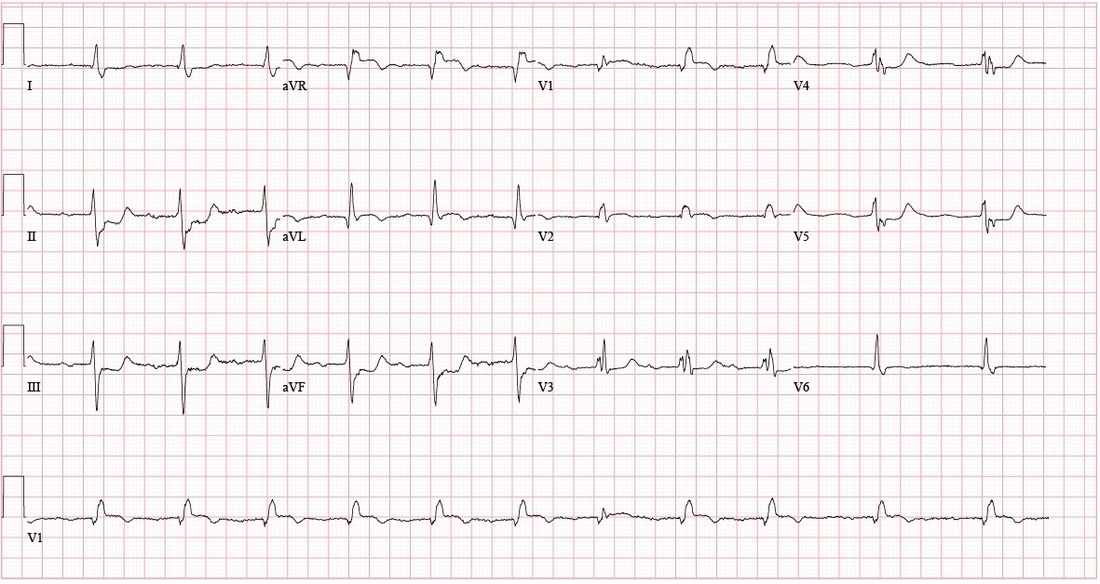 Questions: How is a bifascicular block diagnosed? What are the clinical implications of the bifascicular block? What about in the context of a first degree AV block? ECG Interpretation: Sinus rhythm, rate 69, with sinus arrhythmia and First Degree AV Block. PR interval 272. QRS 150. QTc 490. Left Axis Deviation. (QRS is upward in I and downward in II) Right BBB + Left Anterior Fascicular Block = Bifascicular Block Subtle ST Elevation V1 and V2; consider anterolateral STEMI ST depression inferior leads; inferior ischemia vs. reciprocal changes from anterolateral STEMI Discussion: 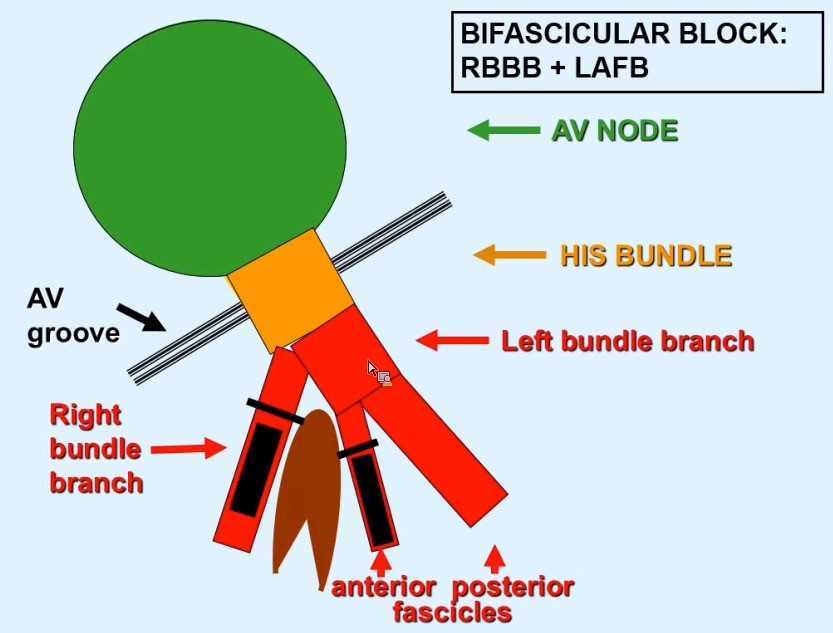 Definitions: (LAFB = Left Anterior Fasicular Block; RAFB = Right Anterior Fascicular Block )
• Bifascicular block: RBBB + either LAFB or RAFB o RBBB + Left Axis Deviation (<-45) = LAFB o RBBB + Right Axis Deviation (>+90)= RAFB • Incomplete Trifascicular block: Conduction damage to all three fascicles o Bifascicular block + first degree AV block OR o Bifascicular block + second degree AV Block OR o RBBB+ Alternating LAFB/LPFB Implications: o In an asymptomatic patient, bifascicular block is largely incidental and no workup is indicated. o If the patient presents with syncope and bifascicular block, this is a medical emergency and the American College of Cardiology and AHA recommend pacemaker implantation. o Risk of progression to complete heart block thought to be low (1% per year in a cohort of 554 patients), but some studies have suggested rates as high as 16% in RBBB + LAFB and 21-75% in RBBB + RAFB. Higher risk in a retrospective review prior to modern reperfusion therapy. o Patients with incomplete trifascicular block are thought to have a greater risk of progression to complete heart block, though data are not conclusive Patient course: Admitted to ICU with systolic pressure in 70s, felt to be cardiogenic shock secondary to MI. Patient was treated with 1 amp of atropine, which improved heart rate from 40s to 70s. Initial troponin was 3.41, which plateaued at 84 on 9/8. No ST elevation. Poor cath candidate given age, AKI at presentation. Treated medically (ASA, statin, Plavix, heparin gtt, carvedilol) and has been transferred to the floor, now hemodynamically stable. Last ECG relatively unchanged since admission (persistent first degree AV block, RBBB, LAFB, ST depression. References: • Dr. Littmann’s ECG Lectures (graphic also from Dr. Littmann) • http://lifeinthefastlane.com/ecg-library/basics/bifascicular-block/ • Uptodate sections on “Conduction Abnormalities after Myocardial Infarction” and “Course and Treatment of Bifascicular Block” • ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices): developed in collaboration with the American Association for Thoracic Surgery and Society of Thoracic Surgeons. Circulation. 2008;117(21):e350. By: Dean Tanner, PGY1
0 Comments
|
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
