|
HPI: The patient is a 71 year old male with PMH of ischemic cardiomyopathy (HFrEF 25%) and AICD in place, moderate mitral regurgitation, permanent atrial fibrillation (rate control and fully anticoagulated), HTN, and COPD who presents to the ED with worsening shortness of breath following a fight with his girlfriend a few hours before. He denies any chest discomfort or palpitations but does endorse presyncope with tunnel vision. At onset, he turned his home O2 up to 3L from 1L. Upon EMS arrival, he received solumedrol and a Duoneb treatment without improvement. Upon arrival to the ED the patient was tripoding and in severe respiratory distress. A trial of BiPap in the emergency department was unsuccessful 2/2 continued distress and increased work of breathing, and the patient was subsequently intubated. Exam: significant for tachypnea to 29. Otherwise VS wnl.. Tripoding and accessory muscle use. Irregularly irregular rhythm with blowing holosystolic murmur 3/6 loudest at the left sternal border. CXR:  - Interpreted as severe pulmonary edema EKG: 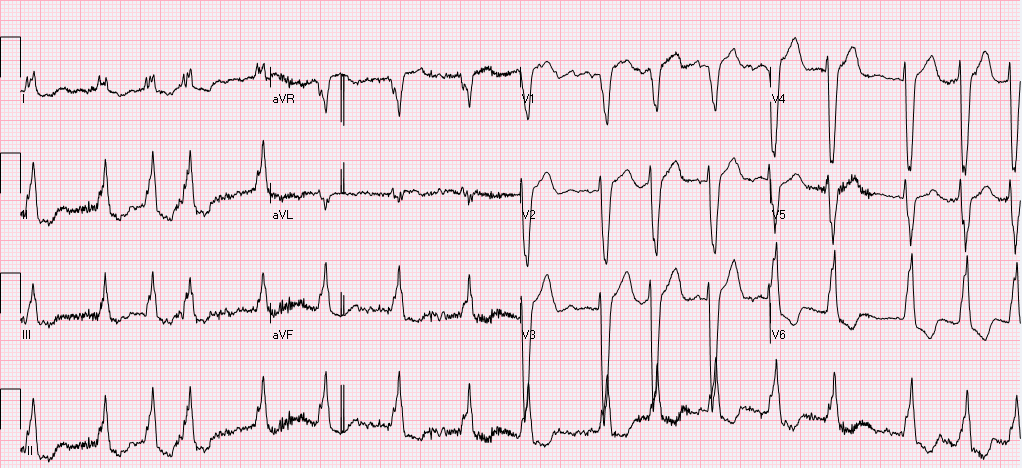 EKG (prior to intubation): Atrial fibrillation. Rate 90’s. Normal axis. QRS >140ms. QS in V1 consistent with LBBB. High frequency oscillatory pattern/respiratory artifact noted as highlighted above, consistent with severe respiratory distress. No Sgarbossa criteria are present. Occasional pacer spike noted.
Relevant Laboratory Data: BNP 1400 from prior 1000, Troponin 0.00à0.06, spot cocaine negative Echo: Left atrium and ventricle are dilated. LVEF 25-30% with septal akinesis. Normal valvular function, however prior echo does report 3+ mitral regurgitation. Otherwise unchanged from prior. Interval History: The patient was admitted to MICU, where he was subsequently weaned from the ventilator and extubated within hours of admission following afterload reduction and IV diuresis. Chart review did demonstrate this to be the third admission in the last 2 months for similar symptoms requiring intubation. Prior AICD interrogations demonstrated afib with RVR with a rate of >200, presumed to be the inciting event for respiratory failure. Current management plan (pending) is for repeat AICD interrogation, and nuclear perfusion stress testing to rule out new ischemia. Subsequently the patient will be converted to a BiV pacer with plans for ablation of the His-bundle which should prevent further episodes of RVR and will result in complete pacer dependence. Teaching Points: Respiratory Artifact
Littman L, Rennyson SL, Wall BP, Parker JM. Significance of Respiratory Artifact in the Electrocardiogram. Am J Cardiol. 2008 Oct 15;102(8):1090-6. doi: 10.1016/j.amjcard.2008.05.061. Epub 2008 Jul 25. Blog by Dr. Jaron Raper
0 Comments
|
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
