|
HPI: 90 y/o woman h/o sick sinus syndrome, AF, and a pacemaker presents with atypical CP. Troponins are negative, CTPA is negative for PE. She denies palpitations, shock-like sensations, or chest wall contractions. Palpated HR corresponds with QRS complexes on the monitor. EKG: 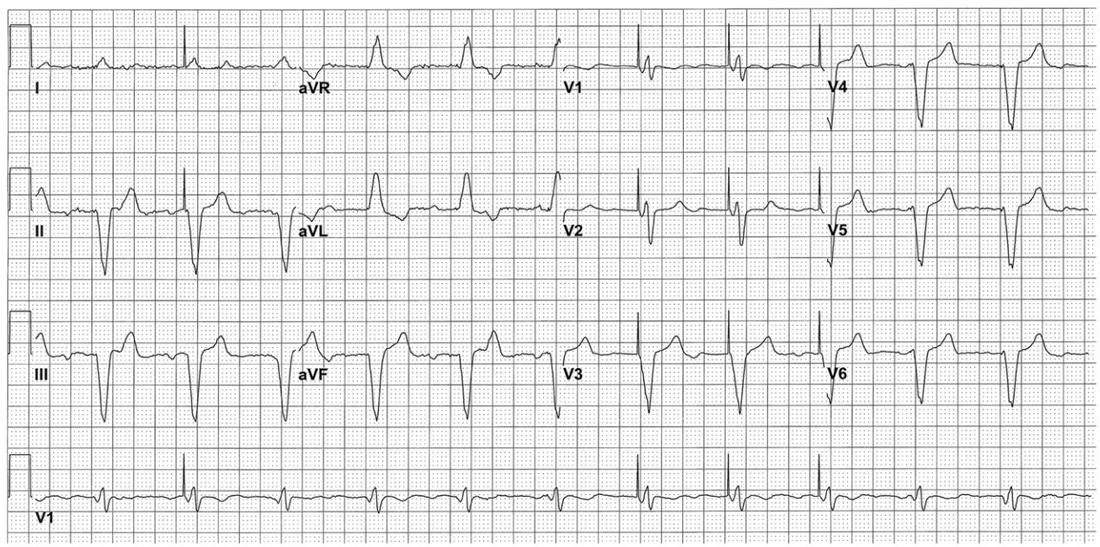 Question:
What's going on with this pacemaker? Is the malfunction the cause of her symptoms? EKG interpretation: Ventricular paced rhythm at a rate of approximately 70. QRS complexes are wide. QRS in V1-V6 are predominantly downgoing as are II, III, and aVF consistent with RV pacing. P waves with variable PR interval are seen in II, III, aVL, aVF, and some of the V leads. Pacer spikes are inconsistently seen in I, II, V1-V3. Discussion: This patient presents with atypical chest pain and an apparent pacemaker malfunction. Her pulse corresponds to her QRS complexes, so what's actually going on? As it turns out, this patient is being paced appropriately at her predetermined rate. Interrogation of her PM revealed normal functionality including normal lead impedance (high impedance can signify a fractured PM wire, low impedance can signify cracked insulation). The issue with the EKG here is that some 12 lead machines pick up small pacer spikes in the surface EKG and amplify them so they are visible to the provider. Unfortunately, some machines will only intermittently detect and amplify these spikes due to their signal processing and occasionally will pick up on interference and amplify it as a pacer spike. If you look closely at aVL, she has tiny pacer spikes before her QRS that the machine did not amplify. In this case, the machine used to record the EKG was a GE Marquette MAC 5000. Note that the QRS complexes in the V1 rhythm strip are all identical despite the intermittent pacer spikes suggesting that the pacemaker is actually generating the impulse for each QRS. Management: - Treat the patient as you normally would... labs, CTPA, ASA, NTG, etc as appropriate - If PM malfunction is suspected, interrogate the device. - Consider machine artifact in a patient with "intermittent" pacing who has consistent QRS complexes on their EKG and an regular HR - CXR can be very useful for identifying pacemaker type and manufacturer; focus on the identification tag on the device By: Dr. Andrew Godfrey, PGY1 References: 1. Butscek R, Farrell RM, Littmann. ECG quiz: what is the cause of the apparent pacemaker malfunction? J Electrocardiol. 2013 Mar-Apr;46(2):108-9. 2. Littmann L, Farrell RM. Potential misinterpretations related to artificial pacemaker signals generated by electrocardiographs. J Electrocardiol. 2015 Jul-Aug;48(4):717-20
0 Comments
|
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
