|
HPI: 20 y/o otherwise healthy male presents after syncopal event while playing basketball. He is athletic, plays basketball 7 days a week, and has never syncopized before. There was a prodromal sensation of “lightheadedness”, but he denies other symptoms and is asymptomatic upon ED arrival. EKG is obtained immediately: EKG: 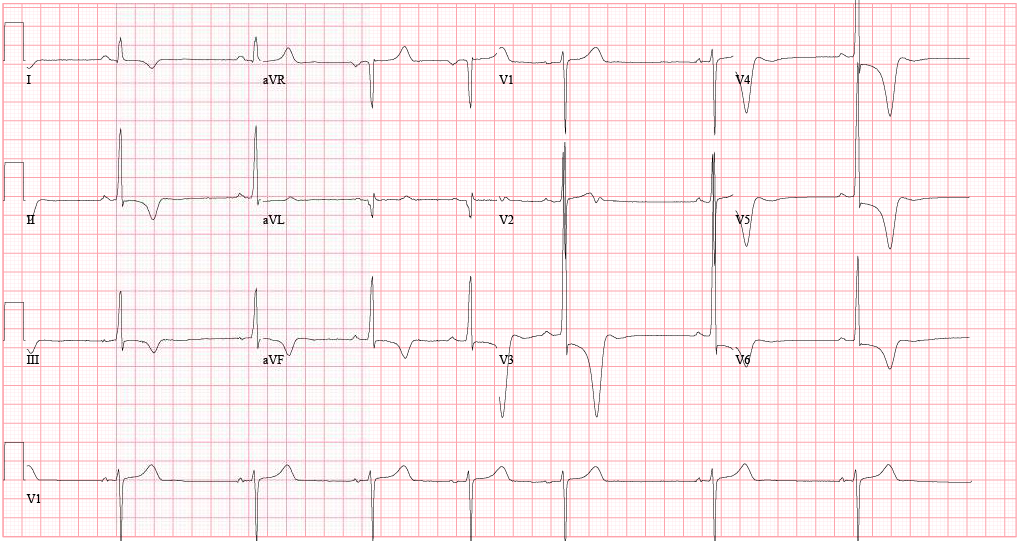 EKG Interpretation:
Sinus bradycardia (46 bpm) w/ profound LVH and repolarization abnormality, diffuse ST depression and T-wave inversions. No prior EKG to compare. Discussion: Large negative T-waves have a broad DDx, including ACS, cocaine toxicity, CNS disorders, metabolic abnormalities, etc. In addition, LVH is a common incidental finding on EKG as well. In a young healthy patient without HTN or aortic stenosis, LVH should raise clinical suspicion for Hypertrophic Cardiomyopathy (HC). Additionally, large deep symmetrical T-wave inversions are typical for the Apical Variant of HC (only 3-5% of total HC cases). Importantly, since there is no LV outflow tract obstruction in this variant, the classic murmur associated with Hypertrophic Obstructive Cardiomyopathy (HOCM) will be absent. Bedside echocardiography confirms the diagnosis. Why is this important? Approximately 1/3 of patients may go on to develop life-threatening complications if untreated. In particular, ventricular arrhythmias. Close monitoring/follow-up is needed, and permanent ICD should be considered. Management: • Continuous cardiac monitoring, ACS evaluation w/ serial troponin and EKGs • Immediate bedside echocardiography • Cardiology consultation and ultimately ICD placement • Longterm avoidance of competitive sports or other intense physical activities By Dr. Blake Johnson References: 1. Siewe D, Nichols K, Furney S, Littmann L. King of Hearts for Ace of Spades: Apical Hypertrophic Cardiomyopathy. Am J of Med. 2014; vol 127 (1): 31-33. 2. Eriksson MJ, Sonnenberg B, Woo A, et al. Long-term outcome in patients with apical hypertrophic cardiomyopathy. J Am Coll Cardiol. 2002;39(4):638-645.
0 Comments
|
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
