|
HPI: Elderly male with history of HTN, DM, and early dementia presents to ED following a witnessed syncopal event at home. Family denies seizure activity, trauma, or anticoagulation. He is now asymptomatic and back at clinical baseline. Laboratory workup and CXR are unremarkable. EKG is shown below: ECG: 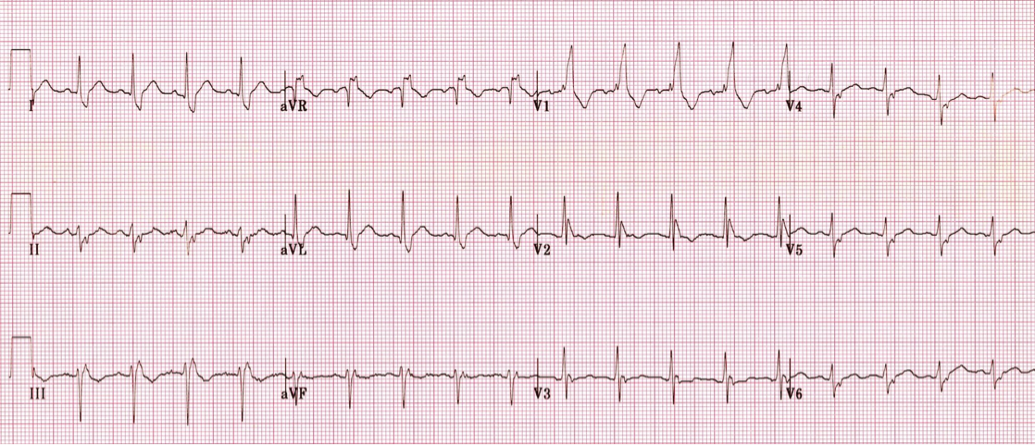 ECG Interpretation: Normal sinus rhythm w/ bifascicular block (RBBB + LAFB). Unchanged from multiple old ECGs dating back more than 8 years. Discussion: Bifascicular block is a combination of Right bundle branch block (RBBB) with either Left anterior fascicular block (LAFB) or Left posterior fascicular block (LPFB). When present, ventricular conduction is dependent on only the single remaining fascicle. EKG findings: · RBBB, and either · Left axis deviation > -45o, or · Right axis deviation > +110o Bifascicular block is a common benign finding. It is indicative of extensive conducting system disease, but risk of progressing to complete heart block is minimal (<1% per year). In isolation, no acute treatment is indicated. HOWEVER, syncope is a red flag! Despite no change from old ECGs, in a patient with known bifascicular block a new finding of syncope can indicate intermittent 3rd degree AV block. Patient is at high risk for PEA arrest, ventricular standstill, and sudden cardiac death. 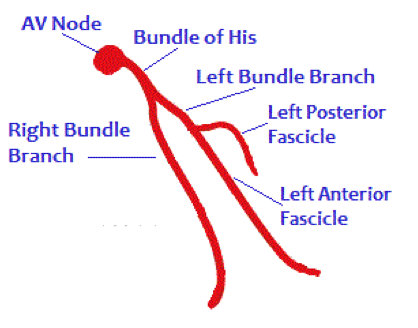 Management:
· Admit to telemetry-monitored floor · Mandatory cardiology consultation · Likely will receive permanent implanted pacemaker By Dr. Blake Johnson References: 1. McAnulty JH, Rahimtoola SH, Murphy E, DeMots H, Ritzmann L, Kanarek PE, et al. Natural history of “high-risk” bundle-branch block: final report of a prospective study. N Engl J Med. 1982 Jul 15; 307(3):137-43. PMID: 7088050 2. Burns, E. Bifascicular Block [Web log post]. Retrieved July 28, 2015, from http://lifeinthefastlane.com/ecg-library/basics/bifascicular-block/
0 Comments
|
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
