|
HPI: Patient is a 54-year-old male presenting with palpitations and near syncope. Patient states that he was told he had a “heart problem” as a child. He was diagnosed with atrial fibrillation some 10+ years ago. EKG: 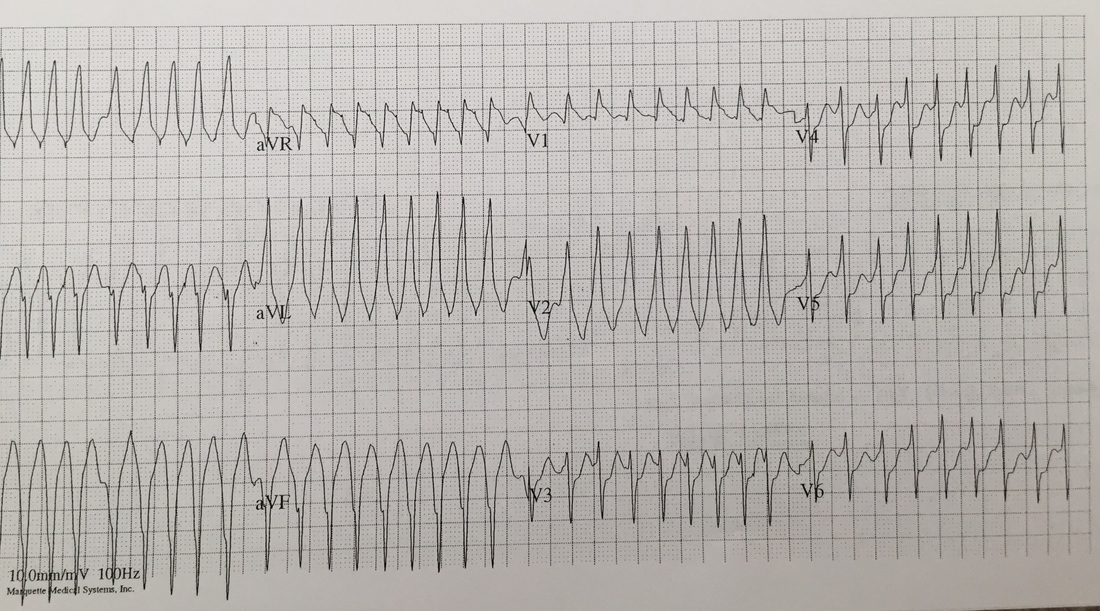 EKG Interperitation:
Rate estimated to be in the high 100s and irregularly irregular. QRS is wide. There are no appreciable P waves. Does not fit any typical bundle branch pattern. Discussion: Is this V tach? No. The patient has a wide complex irregulary irregular waveform. This is MOST likely to be a patient with WPW and a-fib. This is easily confused with ventricular tachycardia. How to differentiate: · Irregularly irregular · Rapid · Wide complex · Does not fit bundle branch pattern · No P waves Treatment: · DO NOT give: adenosine, verapamil, diltiazem, digoxin, beta blocker or amio o Due to the presence of accessory pathway blocking down the AV node, may cause the accessory pathway to become the primary driver of conduction. · Treated with IV procainamide if clinically stable. Dose is 15-16 mg/kg given at a rate no faster than 50 mg/min. · If unstable: Immediate DC cardoversion · Patients will require admission with likely EP study. By Dr Andrew Puchiaty
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
