|
HPI: Approximately 30 year old female with history of frequent PVCs presents via EMS with palpitations and near syncope. She was driving on the highway today when she had to stop due to abrupt palpitations, SOB, and sensation like she was about to “black out”. EKG: 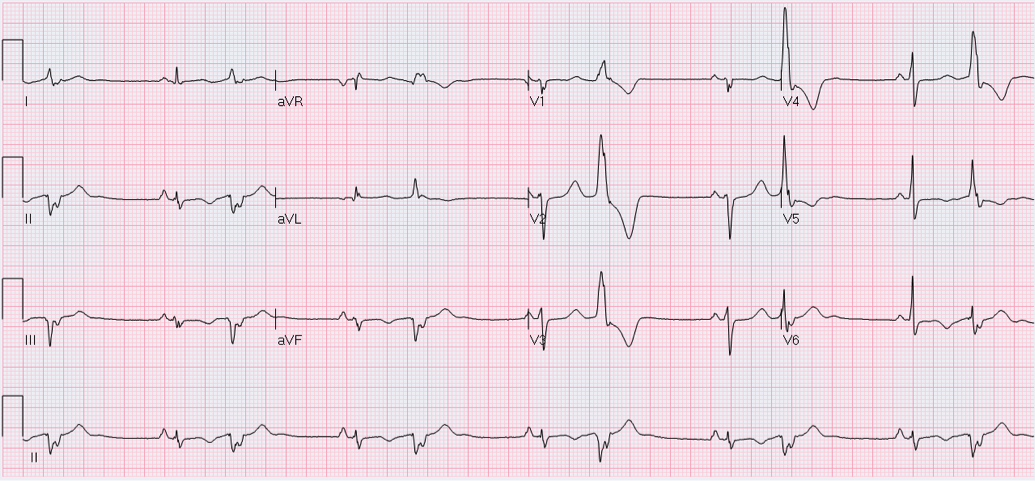 EKG Interpretation:
Sinus rhythm with monomorphic PVCs in pattern of bigeminy. Horizontal axis. Inverted T-waves in inferolateral leads (II, III, aVF, V5-V6). Machine says to consider INFEROLATERAL ISCHEMIA. Discussion: Is this ischemia? No. Patient is young and otherwise healthy with no risk factors for cardiovascular disease. She has a history of frequent ventricular ectopy, and presentation is concerning for transient ventricular tachycardia. Pattern of T-wave inversions is consistent with “Cardiac Memory”. How to differentiate: · Clinical scenario not consistent with ACS · Negative T-waves in same leads where PVCs are negative · Eventual resolution after resumption of normal electrical activation Extent and duration of effect correlates with duration of preceding abnormal ventricular conduction. The longer and more profound the electrical disturbance, the longer and more profound Cardiac Memory persists. Most commonly seen with: 1) Ventricular pacing 2) Intermittent LBBB 3) Pre-excitation in WPW 4) Episodes of ventricular ventricular tachycardia (likely cause in our patient). Management: · High index of suspicion for underlying pathology · Provider awareness of phenomenon so as not to initiate unnecessary interventions (Cath lab, etc.) · Treatment aimed at underlying derangement as appropriate · Inpatient vs. outpatient continuous cardiac monitoring if diagnosis in question By Dr. Blake Johnson
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |
EKG Challenge
AuthorER residents on Dr. Littmann's cardiology service present an interesting EKG and core concepts from Dr. Littmann. Archives
January 2016
Categories
All
Disclaimer: All EKG's and images are the sole property of CMC Emergency Medicine Residency and cannot be reproduced without written consent. Patient identifiers have been redacted/changed or patient consent has been obtained. Information contained in this blog is the opinion of the authors and application of material contained in this blog is at the discretion of the practitioner to verify for accuracy.
|
 RSS Feed
RSS Feed
